- Joined
- Dec 11, 2014
- Messages
- 22,394
- Reaction score
- 29,892
- Points
- 13,841
- Resident [Any Field]

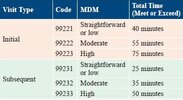
As far as what qualifies for moderate is it similar to outpatient as far a chronic condition with exacerbationSee attachment. 99238 for discharge day if you spent 30 minutes or less on discharge and 99239 if you spent more than 30 minutes. These are all inclusive codes. It's all boring compared to the weirdness of outpatient.
Disagree with the bolded. Many inpatient psych patient easily hit 99233 criteria but can be done in 20 minutes (manic without insight, severe/acute psychosis, severe depression, catatonia, etc). Going mostly based on time is going to undercode a lot of 99233's which is a 0.8 wRVU difference (from 99232) every time it's done. Can make a difference of hundreds or even thousands of wRVUs annually.I would really recommend basing it more on time. Remember that ALL medical specialties use these same exact codes inpatient. But if you want to get into the finer grained details, you can review it here: https://www.ama-assn.org/system/files/2023-e-m-descriptors-guidelines.pdf
This is what I was thinking and why I asked the question, severely ill patients that don’t get actual benefits from spending more than 10-15 minutes with them it definitely seems like billing based on MDM side would be the way to go, but as it falls to psych on inpatient feels less clearly defined to me?Disagree with the bolded. Many inpatient psych patient easily hit 99233 criteria but can be done in 20 minutes (manic without insight, severe/acute psychosis, severe depression, catatonia, etc). Going mostly based on time is going to undercode a lot of 99233's which is a 0.8 wRVU difference (from 99232) every time it's done. Can make a difference of hundreds or even thousands of wRVUs annually.
See attachment. 99238 for discharge day if you spent 30 minutes or less on discharge and 99239 if you spent more than 30 minutes. These are all inclusive codes. It's all boring compared to the weirdness of outpatient.
That would be a terrible strategy for me. Sometimes patients with very complex med regimens need brief check-ins, particularly if they are highly agitated or psychotic. And for less acute patients, my strategy was to spend around 25 minutes with them, but most of that was therapy, after which I have most of the clinical data I need for the E and M and could bill and add-on.I would really recommend basing it more on time. Remember that ALL medical specialties use these same exact codes inpatient. But if you want to get into the finer grained details, you can review it here: https://www.ama-assn.org/system/files/2023-e-m-descriptors-guidelines.pdf
Oh I didn’t know that could be used for an H&P inpatient!Idk where this image comes from but I have never billed a 99223 for an intake on inpatient. I use 90792 and I see no reason why you would not. It's the highest wRVU code available to us (4.16) and can be used multiple days a month/week on frequent fliers.
It can be used in any setting for a new eval. New eval can include ER visits on back to back days.Oh I didn’t know that could be used for an H&P inpatient!
It can be used in any setting for a new eval. New eval can include ER visits on back to back days.
At our hospital the ED 90792 is the admit billing code and first day on unit is a follow up. Not everyone gets seen by psych in the ED though so where end when the admit code is billed varies.I didn't think it could be used in the ER if they end up being admitted. That would mean a 90792 in the ER day 1 and the 90792 the next morning on inpatient. I don't believe that works.
I didn't think it could be used in the ER if they end up being admitted. That would mean a 90792 in the ER day 1 and the 90792 the next morning on inpatient. I don't believe that works.
So our hospital writes a consult note and then an H&P the next day because we can’t bill for resident notes, so the H&P is the first one billed.At our hospital the ED 90792 is the admit billing code and first day on unit is a follow up. Not everyone gets seen by psych in the ED though so where end when the admit code is billed varies.
We use 99223 in the ED, then 90792 the next day on the inpatient unit.At our hospital the ED 90792 is the admit billing code and first day on unit is a follow up. Not everyone gets seen by psych in the ED though so where end when the admit code is billed varies.
We do it the opposite if I see them in the ER. I do the 90792 in the ER and I believe the inpatient docs then does a 99223 the next day (not 100% sure what codes they use though). Not everyone I see in the ER and recommend inpatient admission gets accepted to our inpatient unit (depending on bed availability, behavior on previous admissions, current acuity, or invol status) and sometimes sit in the ER for days before getting admitted somewhere. I can't bill a 99223 for day 1 ER if they're not admitted right away since my ER "follow-up" notes are outpatient codes since the ER is technically an outpatient setting.We use 99223 in the ED, then 90792 the next day on the inpatient unit.
We do it the opposite if I see them in the ER. I do the 90792 in the ER and I believe the inpatient docs then does a 99223 the next day (not 100% sure what codes they use though). Not everyone I see in the ER and recommend inpatient admission gets accepted to our inpatient unit (depending on bed availability, behavior on previous admissions, current acuity, or invol status) and sometimes sit in the ER for days before getting admitted somewhere. I can't bill a 99223 for day 1 ER if they're not admitted right away since my ER "follow-up" notes are outpatient codes since the ER is technically an outpatient setting.
Do you accept pretty much everyone that the ER psych docs say needs admission though? (Or just eval the ER patients yourselves?)Yea this would be a huge fight at our hospital. Us inpatient folks would not be OK giving up 90792's to the ER psych team lol.
Do you accept pretty much everyone that the ER psych docs say needs admission though? (Or just eval the ER patients yourselves?)
Where I'm at inpatient docs turn a significant number of recommended admissions away. So it would kind of hypocritical for them to demand we not use 90792s and then decline half the people we say need admission (since they do not accept any involuntary patients and turn down many voluntary admits).