painquestions8989
Full Member
- Joined
- Jul 10, 2024
- Messages
- 36
- Reaction score
- 26
- Points
- 46
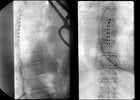
85y F, history of L2-L5 fusion, continued back and leg pain, mild canal stenosis with many disc bulges on MRI. Two days ago SCS trial goes smoothly, 30 mins in and out without issue. Wide awake for testing and most of placement. An hour later get a call from PACU that she is having severe hip and groin pain. Go see her, no real radicular symptoms, strength & sensation intact. Discussed that it's likely from positioning and should get better.
Called her today, still having the same pain, and "electrical sensations" in the legs. Difficulty walking due to pain. No saddle anesthesia or bowel/bladder incontinence. Discussed that the stim settings likely need to be tweaked to stop the paresthesias. Discussed less likely causes (hematoma, cord compression). Discussed an early lead pull at day 5 if her symptoms continue, or go to E.R. if things suddenly worsen.
Given the recent thread about thoracic imaging prior to SCS (which she did not have) wondering if I am missing something and should be pulling these leads today?
Thank you.
Called her today, still having the same pain, and "electrical sensations" in the legs. Difficulty walking due to pain. No saddle anesthesia or bowel/bladder incontinence. Discussed that the stim settings likely need to be tweaked to stop the paresthesias. Discussed less likely causes (hematoma, cord compression). Discussed an early lead pull at day 5 if her symptoms continue, or go to E.R. if things suddenly worsen.
Given the recent thread about thoracic imaging prior to SCS (which she did not have) wondering if I am missing something and should be pulling these leads today?
Thank you.