- Joined
- Dec 18, 2013
- Messages
- 185
- Reaction score
- 47
- Points
- 5,281
- Medical Student
Is there one? I only see Merritt Hawkins top 20 in demand.

Would be easier to compile a list of NOT in demand specialties.
I think rads has changed a ton even in just a year or two, it's back on the upswing. Path is terrible, rad onc has rapidly become terrible, ophtho isn't great but is better than the other two if you don't want to live in a major metro.Can't say much other than I remember coming across some data (probably on here) about a year ago saying path, rads, and ophtho had the worst job markets in that order
I think rads has changed a ton even in just a year or two, it's back on the upswing. Path is terrible, rad onc has rapidly become terrible, ophtho isn't great but is better than the other two if you don't want to live in a major metro.
OP the only specialties that could probably be truly classified as "not in demand" would probably be just Path and Rad Onc. Pretty much every field is in demand once you get away from the coasts and major metro type places.
Diagnostic Radiology in 10 years
If we as a society is successful in autonomous driving in 10 years, replacing dx Radiology is child play.
Sleep sells cpap and accoutrements to patients at greatly inflated feesSleep medicine
With computers and out of country radiologistsDiagnostic Radiology in 10 years
If we as a society is successful in autonomous driving in 10 years, replacing dx Radiology is child play.
With computers and out of country radiologists
You need to have a US medical license to practice medicine in the US.
Computers/AI would be a huge liability until they can read and predict things at least as well as actual radiologists. And they are not licensed physicians, so until laws changed, they would not be able to do anything unless an MD were reviewing everything anyway.
Sunshine radiology NighthawkShould you outsource after-hours and weekend radiology shifts?
Read on to better understand cost, quality, and productivity considerations for whether you should keep after-hours coverage in-house or outsource these services.www.advisory.com
The money goes much farther in those countries. Cheaper to send em there. You and I are saying the same thingNighthawk radiologists have completed US residencies and are licensed in the US. They could very well live overseas-they could live in France or China and read overnight ED scans from the US during their local daytime.
You cannot legally practice medicine in the US without a US medical license. I agree radiology would be the easiest specialty to outsource otherwise, but the outsourcing we’re seeing is done by US-licensed MDs.
Sleep medicine
The money goes much farther in those countries. Cheaper to send em there. You and I are saying the same thing
I'm seriously considering this, but not for the economics of it, moreso because I always wanted to be an astronaut and it sounds ****ing cool.Aerospace medicine.
Diagnostic Radiology in 10 years
If we as a society is successful in autonomous driving in 10 years, replacing dx Radiology is child play.
 www.nature.com
www.nature.com
Nighthawk radiologists have completed US residencies and are licensed in the US. They could very well live overseas-they could live in France or China and read overnight ED scans from the US during their local daytime.
You cannot legally practice medicine in the US without a US medical license. I agree radiology would be the easiest specialty to outsource otherwise, but the outsourcing we’re seeing is done by US-licensed MDs.
Forensic pathology
Unless you're doing research it's a very geographically limited field as a city has to be large enough with enough deaths to even be able to remotely justify hiring someone for such a position (think large and mid sized cities only, so probably less than 100 markets across the country). These locations won't need more than one, maybe two, docs other than the biggest cities like NYC or LA. So maybe a market for 300-400 docs total in the country with a basically saturated job market.

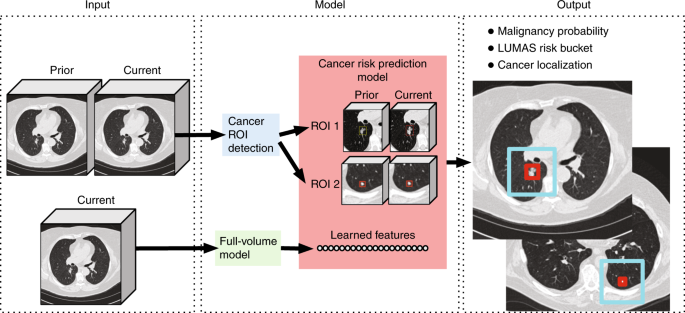
TLDR: They trained a neural network to detect lung cancer on chest CT. Fewer false positives and negatives than human radiologists.End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography - Nature Medicine
A convolutional neural network performs automated prediction of malignancy risk of pulmonary nodules in chest CT scan volumes and improves accuracy of lung cancer screening.
I think people misunderstand machine learning as opposed to hard coded algorithms. The ECG readings are bad because they are hard coded algorithms, not because computers can’t analyze a 2D graph. I work in molecular dynamics research and let me tell you, computers are not bad at looking at 3D images/ analyzing complex data. We have methods now that can analyze protein structure changes that I would not be able to do if you gave me a century. The issue is you need lots of data to make a computer good at a task, much more data than a human would need to be equally good. The lucky thing for the robots is radiographic images are already on a computer, so they have all of the data in the world. I’m not saying DR will be completely outsourced to computers but increasing the efficiency of practicing radiologists (meaning more $$ for those who do this) using neural networks means fewer radiologists will be needed. You don’t have to automate every part of the job to destroy the radiology job market.
Forensic pathology
Unless you're doing research it's a very geographically limited field as a city has to be large enough with enough deaths to even be able to remotely justify hiring someone for such a position (think large and mid sized cities only, so probably less than 100 markets across the country). These locations won't need more than one, maybe two, docs other than the biggest cities like NYC or LA. So maybe a market for 300-400 docs total in the country with a basically saturated job market.
I couldn't disagree with this more. A huge percentage of my patients have significant sleeping problems, many of which are completely unaddressed. You can make a good argument that PCPs should be able to take care of most of this, but many either don't or try several options to no avail. I see a lot of people with refractory sleeping issues and refer to sleep medicine pretty frequently.
Aerospace medicine.
I just did a weekend at the medical examiner in West Palm Beach as part of my M2. They have 7 full-time forensic pathologists, not to mention the tech assistants, and the detectives who work from their office for information gathering.
I just did a weekend at the medical examiner in West Palm Beach as part of my M2. They have 7 full-time forensic pathologists, not to mention the tech assistants, and the detectives who work from their office for information gathering.
I’ve never understood why people think computers will make radiology obsolete anytime in the foreseeable future. We’ve had computers reading ECG’s since the 1970’s, yet we still pay cardiologists to read the ECG’s.
Which provider school did you attend?Kind of proves the point; what other medical field needs just 7 providers to cover 1.5 million people?
What?! I had no idea ophtho wasn’t great, I’m not really interested in it, but just really surprised. How is it still so competitive?
I kid you not, I heard a physician refer to physicians as “medical practitioners”. I can never unhear that phrase.Which provider school did you attend?
How is it a low demand field? People die everyday and I'm pretty sure even those 7 providers can't possibly give out death certificates in a timely manner especially in a place like Florida. In any case, I would bet money that an enterprising individual with training in Forensic Pathology can do very well carving into the coroner's pie if it came down to it.Don't really care about the non-docs, but 7 in west palm is far more than I would have guessed considering I've talked to a forensic pathologist in a large room city that hasn't fewer than that.
Will still stick to my point that it's a low-demand field in general though as this was the consensus among pathologists I talked to when I asked about it.
I am not sure why optho is considered a bad market?
I kid you not, I heard a physician refer to physicians as “medical practitioners”. I can never unhear that phrase.
 www.merriam-webster.com
www.merriam-webster.com
Don't really care about the non-docs, but 7 in west palm is far more than I would have guessed considering I've talked to a forensic pathologist in a large room city that hasn't fewer than that.
Will still stick to my point that it's a low-demand field in general though as this was the consensus among pathologists I talked to when I asked about it.
To clarify it is not a “low demand job.” Many cities have openings and are always hiring. Down here in Miami the ME office does a lecture every year to try and convince people to go into the field.
The problem is it’s a remarkably poor paying job, and not really what most path people want to do. Of the few that do, many leave actual forensic path after a few years to become expert witnesses for the criminal justice system and make more money.
Last I hard starting salary for a forensic pathologist in the city of Miami was ~90k. Which is god aweful for a fellowship trained attending.
How is it a low demand field? People die everyday and I'm pretty sure even those 7 providers can't possibly give out death certificates in a timely manner especially in a place like Florida. In any case, I would bet money that an enterprising individual with training in Forensic Pathology can do very well carving into the coroner's pie if it came down to it.
I would be far more concerned for my job in any non-procedural subspecialty that doesn’t involve imaging, particularly if there’s a “tele-“ option.
Disagree. Telepsych is becoming more and more popular and I've talked to exactly zero psychiatrists who are worried about demand in the field in the next 25 years.