Dermatology
Plastic surgery
Neurosurgery
Otolaryngology
Radiation oncology
I really don't understand how radiology is making your lists. There may be a place for ophtho somewhere on this list, but I'd be hard-pressed to bump one of these.
Not sure if I would put ENT quite on the same level as those others, and instead might put ortho higher (though, like rads, the higher number of positions makes it harder to compare competetiveness of ortho):
plastics
neurosurg
derm
rad onc
ortho
Ophtho could reasonably be included in a top 5 list too, with ENT, uro, and rads following close behind, and in some cases picking up speed.
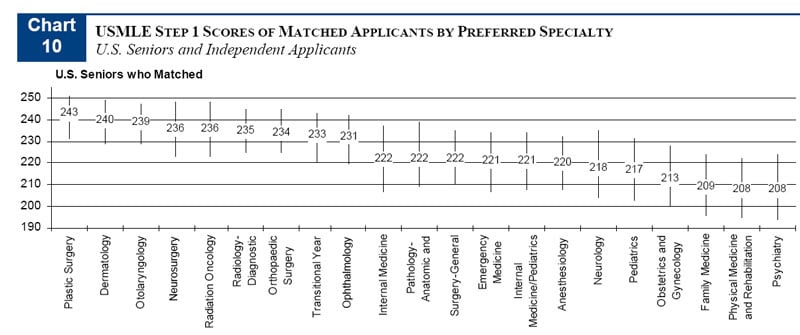
Edit: I guess it really depends on what criteria you go by. According to "Charting Outcomes" the specialties with the lowest match success rate of those ranking them first (not taking into account those applicants who don't even get interviews) goes derm, plastics, ortho, ENT, then rad onc. If you look at Step 1 scores it's plastics, derm, ENT, rad onc, rads. For AOA membership it is derm, ENT, plastics, ortho, rads. For publications it is rad onc, derm, ENT, plastics, ortho. Neurosurg, ophtho, and urology are not included in these data.
Long story short, every specialty has something different they are looking for.