- Joined
- Jan 2, 2009
- Messages
- 1,432
- Reaction score
- 340
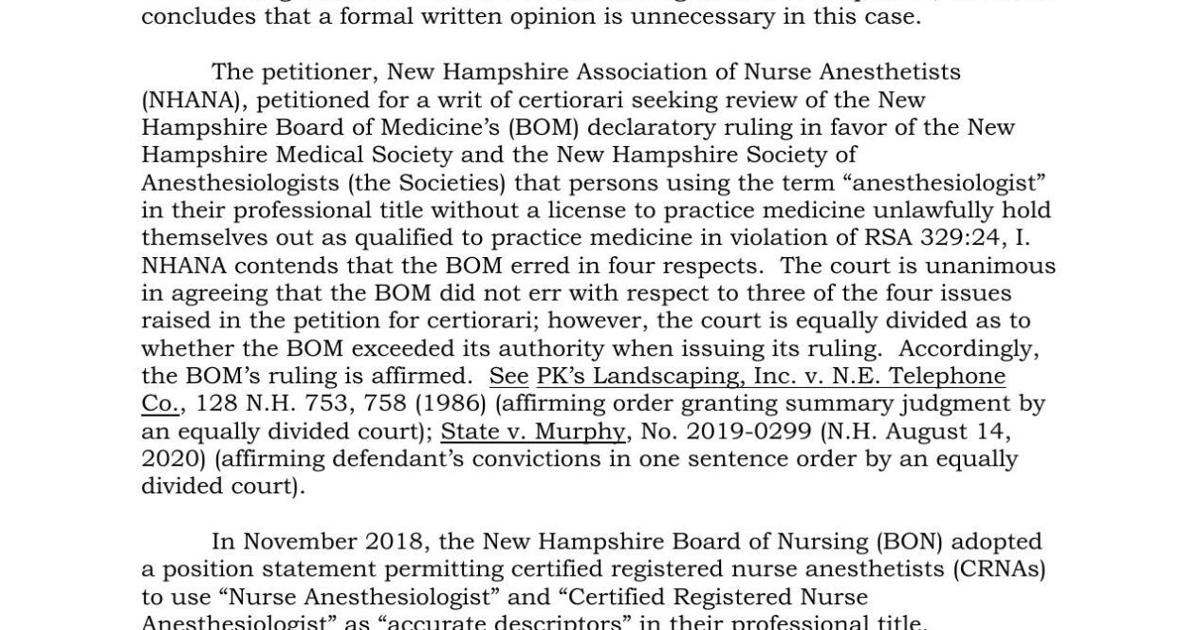
November 20, 2019
American Society of Anesthesiologists Applauds New Hampshire Medical Board’s Prohibition of Medical Title Manipulation
CHICAGO – The American Society of Anesthesiologists (ASA) commends the New Hampshire Board of Medicine’s unanimous vote to prohibit the use of the term “anesthesiologist” unless licensed by the board of medicine.
This patient safety decision comes shortly after lawmakers in Florida prefiled legislation to similarly prohibit the manipulation of the title anesthesiologist, which confuses patients and the public. The New Hampshire Society of Anesthesiologists and the New Hampshire Medical Society worked diligently to protect the public from New Hampshire nurse anesthetists using misleading and manipulated medical titles.
“Patients deserve to know the medical education and licensure of the professional providing their care,” said ASA President Mary Dale Peterson, M.D., MSHCA, FACHE, FASA. “ASA adamantly opposes any effort to confuse or mislead patients through the manipulation of medical titles. We are pleased the New Hampshire Board of Medicine put patients ahead of the political maneuvering of some individuals.”
Earlier this year in New Hampshire, the Board of Nursing released a position statement authorizing use of the optional descriptors “nurse anesthesiologist” and “certified registered nurse anesthesiologist.” The board action occurred without any formal rules process or public comment period. Since that time, the New Hampshire Society of Anesthesiologists, New Hampshire Medical Society, ASA, and American Medical Association have strongly opposed the nursing board’s action and urged it to rescind its inappropriate position statement.
ASA congratulates the New Hampshire Board of Medicine on its efforts to protect patients and the public.
American Society of Anesthesiologists Applauds New Hampshire Medical Board’s Prohibition of Medical Title Manipulation
CHICAGO – The American Society of Anesthesiologists (ASA) commends the New Hampshire Board of Medicine’s unanimous vote to prohibit the use of the term “anesthesiologist” unless licensed by the board of medicine.
This patient safety decision comes shortly after lawmakers in Florida prefiled legislation to similarly prohibit the manipulation of the title anesthesiologist, which confuses patients and the public. The New Hampshire Society of Anesthesiologists and the New Hampshire Medical Society worked diligently to protect the public from New Hampshire nurse anesthetists using misleading and manipulated medical titles.
“Patients deserve to know the medical education and licensure of the professional providing their care,” said ASA President Mary Dale Peterson, M.D., MSHCA, FACHE, FASA. “ASA adamantly opposes any effort to confuse or mislead patients through the manipulation of medical titles. We are pleased the New Hampshire Board of Medicine put patients ahead of the political maneuvering of some individuals.”
Earlier this year in New Hampshire, the Board of Nursing released a position statement authorizing use of the optional descriptors “nurse anesthesiologist” and “certified registered nurse anesthesiologist.” The board action occurred without any formal rules process or public comment period. Since that time, the New Hampshire Society of Anesthesiologists, New Hampshire Medical Society, ASA, and American Medical Association have strongly opposed the nursing board’s action and urged it to rescind its inappropriate position statement.
ASA congratulates the New Hampshire Board of Medicine on its efforts to protect patients and the public.