- Joined
- Jun 18, 2005
- Messages
- 1,916
- Reaction score
- 13,918
No seriously the fortune and fame would be indescribable. Seize your destiny!Most of the docs only attack here without giving an explanation.

No seriously the fortune and fame would be indescribable. Seize your destiny!Most of the docs only attack here without giving an explanation.
Can you be serious with me, please?No seriously the fortune and fame would be indescribable. Seize your destiny!
Based on the evidence at hand, I don't see that happening.Can you be serious with me, please?
Does anyone have an educated guess on this? Have some interest in this, but not if it goes by the wayside. Thoughts?
I mean look to anesthesia and the rise of CRNAs. Anesthesiology isn't gone, but the numbers needed to staff certain floors has gone way down now that you can just have one gas doc supervising a dozen CRNA rooms each doing routine GI scoping.
The setup I'm describing is what I saw on the outpatient GI floor I worked on for a year. What's the most colonoscopy rooms you've known one anesthesiologist to supervise?I’ve been practicing anesthesia for over 20 years. This is not actually a thing. No anesthesiologist supervises a dozen CRNAs.
We need more anesthesiologists now than ever before and there are currently more anesthesiologists practicing than ever before. For the next 2-3 decades we will need more anesthesiologists than we have ever needed in the past. This is just demographics. How to pay for all this is the big challenge.
The setup I'm describing is what I saw on the outpatient GI floor I worked on for a year. What's the most colonoscopy rooms you've known one anesthesiologist to supervise?
Maybe this was just a particularly chill gig for the gas, but yeah it was 100% more than 4:1, and since each GI doc was doing a couple EGDs or colonoscopies per hour it was indeed dozens and dozens and dozens of people moving through in a dayI haven’t heard of an anesthesiologist supervising more than 4 rooms at one time. Even that is taxing. Was that anesthesiologist doing over a hundred preops a day while simultaneously supervising 12 rooms?
Maybe this was just a particularly chill gig for the gas, but yeah it was 100% more than 4:1, and since each GI doc was doing a couple EGDs or colonoscopies per hour it was indeed dozens and dozens and dozens of people moving through in a day
State of the art. *bum dum tssss*Insane. What state was this if I may ask?
MissouriInsane. What state was this if I may ask?
Another issue not often talked about is there has been a significant investment by IBM and others to have AI analyze vitals, labs, symptoms and the rest of the HPI to come up with not only a likely diagnosis but also treatment suggestions based on the current literature. That level of AI only really needs a mid-level in order to implement good care, especially in this day and age where medicine has become more and more algorithmic.
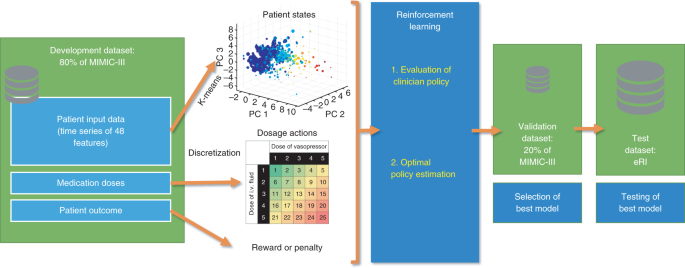
We demonstrate that the value of the AI Clinician’s selected treatment is on average reliably higher than human clinicians. In a large validation cohort independent of the training data, mortality was lowest in patients for whom clinicians’ actual doses matched the AI decisions. Our model provides individualized and clinically interpretable treatment decisions for sepsis that could improve patient outcomes.
 www.nature.com
www.nature.com
Doesn't rads also have procedures? Also, would be so kind and share with us what specifically the general flaw is with the studies?Radiology is the most obvious application for ML/AI due to its digital and easily accessible data. When pathology slides get their own PACS, derm lesions get standardly photographed and stored in the chart, and retina images become more commonplace then all of those fields immediately succumb to the same issue with AI, which would certainly happen. Another issue not often talked about is there has been a significant investment by IBM and others to have AI analyze vitals, labs, symptoms and the rest of the HPI to come up with not only a likely diagnosis but also treatment suggestions based on the current literature. That level of AI only really needs a mid-level in order to implement good care, especially in this day and age where medicine has become more and more algorithmic.
Ultimately my point is that unless you go into a procedure-based field this threat will continue to exist for way more than just radiology. However having read most of the AI radiology studies up to this point, there has been a major flaw in the study designs which drastically limit its external validity (and why often they get published in throwaway journals). I am curious to read this most recent paper in Nature and do think screening will be the first automated task by a radiologist to get implemented. From my discussions with experts in this arena, I am not worried about AI/ML displacing radiologists anytime soon.
Doesn't rads also have procedures? Also, would be so kind and share with us what specifically the general flaw is with the studies?
What about IR?Yes, but makes up a small percentage of their time/compensation.
Many of these studies train their AI using a dataset then use studies from that same dataset to compare to a radiologist. Often it’s not looking at a novel image, which is precisely what happens in practice.
What about IR?
What about IR?
What does IR really do? When I read "International Radiology" I don't know what to think....What about it? Yes IR is procedure-based. It’s trying to separate itself from diagnostics. When most people use “AI” and “Radiology” together they almost always mean Diagnostic Radiology and not IR.
Yes, but makes up a small percentage of their time/compensation.
Many of these studies train their AI using a dataset then use studies from that same dataset to compare to a radiologist. Often it’s not looking at a novel image, which is precisely what happens in practice.
The AI was providing an assessment of the images that they trained on as opposed to being given new images. It's like giving your students homework and then copying and pasting the homework and calling it the test.What are you talking about?
“Not looking at a novel image” - what precisely do you mean?
What does IR really do? When I read "International Radiology" I don't know what to think....
The AI was providing an assessment of the images that they trained on as opposed to being given new images. It's like giving your students homework and then copying and pasting the homework and calling it the test.
Exactly
Pardon, voice-to-text while walking without doing a double check. Meant interventional. Also, I did not know that. I imagined radiology as black room people and thus have avoided the topic. I will look in to this as my progress through schooling progresses because this specialty sounds....Rad.IR = Interventional Radiology.
Minimally-invasive, image guided procedures treating a wide variety of conditions.
What IR does on a day-to-day basis can range from acting like a surgical service: rounding on inpatients, doing high-end oncologic and vascular cases, treating emergencies etc, but can be as sleepy as doing 60% diagnostics and doing basic procedures (thoracentesis, paracentesis, ports, fibroids etc).
Society of Interventional Radiology - Residents, Fellows, and Medical Students
This is an exciting time to pursue a career in interventional radiology. There are over 2,000 SIR In-Training Members from all over the world. We invite you to become a member of SIR, learn about interventional radiology, and play a role in the development of the specialty.www.sirweb.org
No, none of the studies being cited regularly did this.
If you have an example of a study that did this, either you are mistaken or it should be retracted.
It’s trivial to get 100% accuracy on any training set in machine learning just by overfitting.
There are different issues with many of the studies out there, but this is not one of them.
No, not “exactly”.
You either do not know how to read these papers or have zero familiarity with the literature.
6 years of residency? Let me do a rotation in it before saying anything else lolIR = Interventional Radiology.
Minimally-invasive, image guided procedures treating a wide variety of conditions.
What IR does on a day-to-day basis can range from acting like a surgical service: rounding on inpatients, doing high-end oncologic and vascular cases, treating emergencies etc, but can be as sleepy as doing 60% diagnostics and doing basic procedures (thoracentesis, paracentesis, ports, fibroids etc).
Society of Interventional Radiology - Residents, Fellows, and Medical Students
This is an exciting time to pursue a career in interventional radiology. There are over 2,000 SIR In-Training Members from all over the world. We invite you to become a member of SIR, learn about interventional radiology, and play a role in the development of the specialty.
6 years of residency? Let me do a rotation in it before saying anything else lol
Interesting - Not to hijack the thread but what is the day-to-day life of Radiology residency and attending?All of radiology is essentially 6 years (typically DR training 1 yr internship + 4 residency + 1 fellowship).
Some subspecializations even more (NIR is typically as long as neurosurgery, which I suppose is fitting).
Interesting - Not to hijack the thread but what is the day-to-day life of Radiology residency and attending?
And it sounds like most everyone does some form of fellowship after DR?
Interesting. Looking more in to IR it seems like the closest you can get to surgery without actually having to do surgery, and a nice diagnostic aspect to it too. Will try to reach out to see if there are any in my area I can shadow.Almost everyone does a fellowship.
Day to day varies by type of practice, but is mostly reading in most places.
All radiologists get procedural training and most still do occasional procedures, both DR and IR, but varies by degree of subspecialization of group.
Interesting. Looking more in to IR it seems like the closest you can get to surgery without actually having to do surgery, and a nice diagnostic aspect to it too. Will try to reach out to see if there are any in my area I can shadow.
Be forewarned that integrated IR has the lowest match rate of anything right now - 58% success rateInteresting. Looking more in to IR it seems like the closest you can get to surgery without actually having to do surgery, and a nice diagnostic aspect to it too. Will try to reach out to see if there are any in my area I can shadow.
Be forewarned that integrated IR has the lowest match rate of anything right now - 58% success rate
Next lowest after that is Dermatology at 82%
So huge numbers of people hoping to do IR still have to go the old school route of a full DR training first, then additional fellowship time
I can see why, cool procedures based specialty with good work life balance and a $400,000 salary. pretty dope. But alas, I am merely an MS(-1) and have 4 more years to worry about being competitive for Match day.Be forewarned that integrated IR has the lowest match rate of anything right now - 58% success rate
Next lowest after that is Dermatology at 82%
So huge numbers of people hoping to do IR still have to go the old school route of a full DR training first, then additional fellowship time
Thoughts on whether both pathways will remain, or whether it'll all collapse into integrated style like we've seen with Plastic surgery?There’s still an additional entry point from DR:

Independent IR residency with Early Specialization in Interventional Radiology (ESIR)
Early Specialization in Interventional Radiology (ESIR) is a training option for diagnostic radiology residents and medical students who identify an early desire to specialize in interventional radiology.www.sirweb.org
As long as you go to one of the residencies with an ESIR track, you can still become an interventional radiologist (if you don’t have too much competition within your residency).
Trust me dude the worry begins Week 1 when everyone starts selling their souls to ZankiI can see why, cool procedures based specialty with good work life balance and a $400,000 salary. pretty dope. But alas, I am merely an MS(-1) and have 4 more years to worry about being competitive for Match day.
Never have used flashcards and never will. I am all about learning and not memorization. If that means just doing OK then I am totally cool with PM&R or Path.Trust me dude the worry begins Week 1 when everyone starts selling their souls to Zanki
Thoughts on whether both pathways will remain, or whether it'll all collapse into integrated style like we've seen with Plastic surgery?
Trust me dude the worry begins Week 1 when everyone starts selling their souls to Zanki
Never have used flashcards and never will. I am all about learning and not memorization. If that means just doing OK then I am totally cool with PM&R or Path.
Yeah I friggin hate flashcards too, but in hindsight it would've been the way to go for anatomy, biochemistry, and microbiology units. There's just no way to think your way to the answer of a question like, "is bug X catalase positive or not"
At least for micro I have the benefit of having worked as a lab tech in a medical laboratory for the last 6 years (3 of which included micro rotations/duties)....Yeah I friggin hate flashcards too, but in hindsight it would've been the way to go for anatomy, biochemistry, and microbiology units. There's just no way to think your way to the answer of a question like, "is bug X catalase positive or not"
At least for micro I have the benefit of having worked as a lab tech in a medical laboratory for the last 6 years (3 of which included micro rotations/duties)....
Although you can associate "This organism is an obligate aerobe, thus it likely is catalase positive" knowing that catalase is utilized in the conversion of Oxygen free radicals in to (H2O2....?) I know that is just an example, but you get whereI am coming from. And I get where you are coming from. Maybe not flashcards but drawing out the whole thing labeling along the way. IDK, I will figure it out when I get there!
Never have used flashcards and never will. I am all about learning and not memorization. If that means just doing OK then I am totally cool with PM&R or Path.
Almost everyone eventually comes to the dark side, even if it is just for certain topics. There is a lot in medicine, pre-clinical years especially, that is simply brute memorization and unable to be reasoned through. Zanki (substitute "spaced repetition" here if you want) is much more learning than people realize. It's like doing a massive puzzle. While at first it feels like laying down random pieces and factoids, eventually you step back and realize you have pieced together a Rembrandt.
Any advice for a good strategy for creating cards?
Jealous of the material for medical students but each time I start I generate way too many and don’t stick with it.
So just like my early example of self driving cars, the issue for the foreseeable future is not the job or technology itself but the humans that job/technology interacts with.AI will make radiologist jobs more efficient, but it will never replace them.
Nor will it replace any of the rest of us. I think my own field is probably the simplest example: Half my job is diabetes. Diabetes treatment actually isn't that complicated. There's 12 classes of drugs - but even if you split out every single insulin as its own agent, there's <50 options, most of which are only available in 1-3 doses (except insulin of course). A good number of them are useless, so once you pared that back you could come up with a flow chart that would do a pretty easy job approximating my decisionmaking process for what my preferred agent is for any given situation (taking into account comorbidities, drug-drug interactions, hell, even cost/coverage potentially). I could probably train a motivated high school student a couple weeks to review all that information and treat my patients (though insulin titration, particularly for a type 1, would probably require a bit more training). An AI neural net would do even better than that.
And both would fail at figuring out not what the best option is but the best option the patient is willing to take. Or convincing the patient to take shots. Or if the patient is hesitant, bargaining with them on the amount of shots they're willing to take.
There's a strong human component where an empathetic, trained physician sitting down and discussing the patient care cannot be beat. No computer will be able to do that in any conceivable timeline - the patients just won't go along with it.
Right. Medicine would be really simple if it weren't for all those patients.So just like my early example of self driving cars, the issue for the foreseeable future is not the job or technology itself but the humans that job/technology interacts with.