- Joined
- Mar 7, 2012
- Messages
- 94
- Reaction score
- 3
A new NBME 15 is out! Here is the official discussion page. How did you guys feel about this nbme?

.I think you guys are just over thinking this. DKA, too much glucose in the blood correct, that isn't getting taken up. Glucokinase is inducible, hence why it has a high Vmax, by insulin. This was the logic that I used, and in addition going back to my previous argument, all the other enzymes listed would only make the situation worse since they would lead to an increase glucose levels in the blood.
-Hi guys, was wondering if I could get some help on some of the questions. A brief EXPLANATION would be great too if you have one.
Before I post though, I briefly read some of the above posts and thought I'd contribute:
- I got the Down Syndrome with ALL wrong too. I put MEGALOBLASTOSIS because of pathoma. But note that Megaloblastosis DOES NOT refer to Megakaryoblastic Leukemia, it refers to large RBC's (MCV>100). So I guess pathoma isn't wrong in this case.
- saw someone post that the anal lesion with a picture was SCC of the anus, but its actually external hemorrhoids (painful and doesn't bleed). Maybe someone already corrected this.
My questions:
Lymphocyte neoplasm DOES NOT express: CD4, CD8, surface igM, surface IgG, cytoplasmic IgM and mu-heavy chains, cytoplasmic IgG, and gamma-heavy chains. It DOES express class I MHC and show rearrangement of the T-lymphocyte receptor beta-chain gene D and J segments. Which is the normal counterpart?
a. Activated cytolytic effector T lymphocytes in circulation
b. Mature IgM-secreting B lympchotes in LN
c. Mature Immunoglovulin secreting plasma cells in LN
d. Pre-B lymphocyte progenitor of mature B lymphobytes in the BM
e. T-lymphocyte thyocytes localized to the thymic cortex
This is a double negative immature T cell that localizes to the thymic cortex
Kid presents with congestive heart failure due to a VSD. After fixing the VSD, what changes will be seen in the following:
- Left Ventricular P
- Right Ventricular P
- Left Atrial P
LV pressure increases, RV pressure decreases, and LA pressure decreases. The left to right shunt from LV to RV is driving the pressure in the LV down, and since the RV is getting an increased volume of blood the pressure in the RV is greater. This increased volume is then transmitted through the LA. The pressure doesnt drop until the LV when it all repeats again
Pls help :
1.The question of the 25 yrs old man participating in the muscle function study ..3 columns were put with : epp-Amplitude , mepp- Amplitude and response in mV to Ach .
Based on the normal values the question asked about the muscle Bx specimen in Acute botulism
I answered A which was wrong .
I am not good in experiment questions ... .
6.During the experiment of muscle contraction intracellular Ca is decreased after a substance is adm .The question asks WHY contraction is inhibited in this case .
I answered E which was wrong .
Somebody with a better idea ?
Much appreciated .
look at that muscle study question...because i know for a fact there was another option that had the value of 1 as the answer choice for Ach on the far right hand side...can you just post up a link to the question?
OK ,So the muscle study question :
Normal muscle epp Amplitude 10, mepp Amplitude 1 , Response in (mV) to ASch 1 .
The answeres options we are looking at are :
epp amplitude 1 , mepp Amplitude 1 ,Response in( mV) to Ach 1
or
epp Amplitude 15 , mepp Amplitude 1 , Response in (mV) to Ach 1 .
Which one do we chose after Botulinum administration ?
I can not do more explicite due to copyright ...
Thanks a lot .
.
OK , Glukokinase is affected positively by Insulin .
I know that as a fact working in ICU with Ketoacidosis patients .
Second reason is that Glukokinase mutation is responsible for MODY ( mature onsetT DM of the young) . And this is also a fact .
Its the first one. botulism blocks ach release, but it has no effect on mepp because these are normal random quantum fluctuations of ach in the synapse. Like wise botulism, blocking ach release has no effect on voltage difference response. The voltage difference is dependent on other factors such as membrane potential and ion concentrations.
I forget the answers to the other 2. So someone else can chime in
There was a question about a premature baby with respiratory distress and it asked which of the following parameters would INCREASE?
alveoli radii
lung complience
lung elastic recoil
pleural pressure
surfactant secretion
Obviously it is not surfactant secretion, lung elastic recoil, and I didnt think it was pleural pressure. I was between lung complience and alveoli radii. I put lung complience which was wrong. So is it alveoi radii? I know the radius of some alveoli increases, but at the same time other alveoli collapse...
I think I had lung elastic recoil and i didn't get it wrong...
hmm thats interesting. any idea on the mechanism?
I think that question is just gearing you towards ARDS of a newborn ---> hyaline membrane ---> restrictive
not saying that your answer is wrong, but the way I thought about it was
ARDS due to decreased surfactant--> Increase tension --> alveoli want to collapse (P =2T/r) P = collapsing pressure
hmm thats interesting. any idea on the mechanism?
not saying that your answer is wrong, but the way I thought about it was
ARDS due to decreased surfactant--> Increase tension --> alveoli want to collapse (P =2T/r) P = collapsing pressure
I think I had lung elastic recoil and i didn't get it wrong...
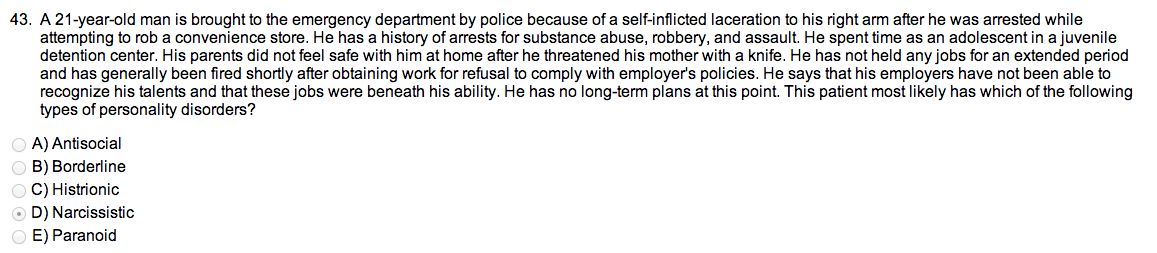
what was the personality behavior of the one patient? i wrote narcissistic...but that obviously was wrong...
was it antisocial? reviewed the personality disorders, and it seems to be the one that fits.
Yup I answered antisocial and it wasn't marked wrong for me! I think the "feeling jobs were beneath his ability" throws you towards narcissistic, but the whole no regard for authority sways the answer more towards antisocial.
Alright, my two questions:
Woman comes in who obviously has somatization disorder. What's the question that you want to ask her?
Is it: "I'd like to assess the symptom causing you the most distress and schedule a monthly follow up appointment."?
The other one was the phenylalanine hydroxylase one. The PH gene was homozygous for a point mutation in intron 12 (GT->AT) that causes skipping of exon 12. What causes the skipping of exon 12?
a- alternative polyadenylation site
b- deletion of 5' untranslated region
c- expansion of trinucleotide repeat
d- gene duplication
e- nonhomologous recombination
f- not it
g-RNA splice error
h- X inactivation
Alright, my two questions:
Woman comes in who obviously has somatization disorder. What's the question that you want to ask her?
Is it: "I'd like to assess the symptom causing you the most distress and schedule a monthly follow up appointment."?
yup...i recall that one of the answers was blatantly wrong, which was the last option...you never refer them to another physician...if you list the other choices...i can tell you why they're wrong
edit: how do you go about solving that 2nd question...hate questions pertaining to molecular techniques...
Phew this one was tough. Going over it now so I'll surely have a few questions coming up (and I'm trying to search the thread to make sure I don't repeat questions... bear with me people). The first one is about the autosomal dominant pedigree that skips the mother. On a different NBME, I literally saw the exact same pedigree and it was variable expressivity. Not the case on this one... I'm guessing it was incomplete penetrance (both were answer choices on both questions).
The variable expressivity was in reference to NF1 while this question was about Hereditary Telangiectasia. Do we just have to memorize which diseases are which and accept the fact that the pedigrees can look the same?
Tx of lady with exposure to radioactive I?
Levothyroxine
Liothyronine
Propylthiouracil
Methimazole (my choice - wrong)
Potassium Iodine
I was thinking this or PTU to prevent the organification and formation of radioactive Thyroid hormone. Maybe PTU was right I don't know. Am I missing something here?
Tx of lady with exposure to radioactive I?
Levothyroxine
Liothyronine
Propylthiouracil
Methimazole (my choice - wrong)
Potassium Iodine
I was thinking this or PTU to prevent the organification and formation of radioactive Thyroid hormone. Maybe PTU was right I don't know. Am I missing something here?
Nice, thanks guys! So essentially it works in a somewhat similar fashion to the anions (perchlorate and -technate) since they comp inhibit the Na/I symporter?
I ask because I want to understand the concept completely. If perchlorate was a choice and KIodine wasn't it would be the correct answer also right?
Cool stuff. Thanks.and i also got the top one wrong
Metronidazole. It's Trichomonas vaginalis.Female with non-foul, non-fishy STD with frothy yellow green discharge from the vagina with red spots on cervix and motile organisms with flagella. How do you treat?
IM Pen G
IV Ceftriaxone and oral doxy
Metronidazole
or an antifungal?
I couldn't figure out if what organism they were asking here
Hah, I put that last option. And yes I feel bad about it.yup...i recall that one of the answers was blatantly wrong, which was the last option...you never refer them to another physician...if you list the other choices...i can tell you why they're wrong
edit: how do you go about solving that 2nd question...hate questions pertaining to molecular techniques...
Phew this one was tough. Going over it now so I'll surely have a few questions coming up (and I'm trying to search the thread to make sure I don't repeat questions... bear with me people). The first one is about the autosomal dominant pedigree that skips the mother. On a different NBME, I literally saw the exact same pedigree and it was variable expressivity. Not the case on this one... I'm guessing it was incomplete penetrance (both were answer choices on both questions).
The variable expressivity was in reference to NF1 while this question was about Hereditary Telangiectasia. Do we just have to memorize which diseases are which and accept the fact that the pedigrees can look the same?
Introns are taken out using snRNPs specific to certain splice sequences. RNA splicing is really the only association with intron/exon problems.
what'd you think about this exam? did you already go through 11, 12, and 13...

Metronidazole. It's Trichomonas vaginalis.
I can only compare it to 12 and the one our school gave us (which was incredibly easy), but I thought this was way harder than 12. Got the exact same score in the end but missed 4 more questions.
I'm ok with it because on this one I didn't make any stupid mistakes... each of the ones I got wrong were straight up things I either never learned or the question was written poorly, so at least my testing skills have improved if my general knowledge hasn't
yeah this one was kinda hard...i didnt know colorectal carcinoma metastasizes via hematogenously...i only thought it was the ones mentioned in pathoma...
even that other question that had the frameshift mutation...an additional C is inserted...but none of the answer choices made sense...got that wrong
got the NY/SF question wrong, but got the botulisum question right...
i hope the step isn't as difficult as 15...
edit: imo, 11 = 12 > 13 >> 15 from easiest to difficult...emphasis on the two >'s from 13 to 15...lol...i'd say 13 is only a fraction/tad bit harder than 11 and 12