- Joined
- Mar 7, 2012
- Messages
- 94
- Reaction score
- 3
A new NBME 15 is out! Here is the official discussion page. How did you guys feel about this nbme?

I think it's bethanechol. They're asking for something that stimulates Gq, which would increases PI turnover (aka a muscarinic agonist) that isn't a nicotinic agonist. The rest of them are either antagonists or act on nicotinic receptors.Can anyone help with this one: A drug that increases phosphoinositide turnover, but does not affect nicotonic synapses?
Atropine, Bechanecol, neostigmine, succinylcholine?
Really confused on this one.
So is this a toxoid vaccine which means its a purified inactivated toxin?
Ceftriaxone is beta lactamase stable.
thanks.+1
The whole point of using cephalosporins is that they're almost impossible for beta lactamases to degrade. Ampicillin, on the other hand, is more easily degraded by beta lactamases. The difference between these drugs makes E the right answer.
Everyone is in the same boat during their prep. Now hopefully you will remember that ceftriaxone is useful against beta lactamase producing species, and maybe you'll even see if there are other similar beta lactams.thanks.
I feel like no matter how much I study, i still miss stuff that everyone else knows. arrg
Can anyone explain why deoxyHb being a better buffer of hydrogen ions than OxyHb allows deoxygenated blood to carry more CO2 than oxygenated blood?
I feel like that's a basic question but for some reason I'm just not making the connection of how that is linked. Would really appreciate an explanation!
does it have to do with the haldane or bohr effect or is it a simple fact...not sure why this isn't clicking with me ...thanks for the reply though !it changes conformation so that it can bind hydrogen better
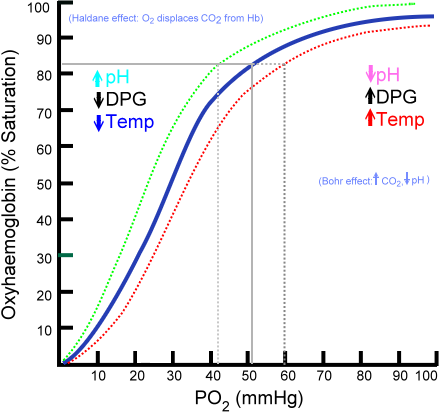
haldane effect: deoxygenated blood can hold carbon dioxide better as carbaminohemoglobin, attached to hemoglobin
bohr effect means that hemoglobin can bind oxygen better or worse depending on various factors. it's basically when you see the curve right shifting on the po2/oxyhemoglobin curve due to increased h+, temp, dpg, co2
These phenomena are not very relevant to your question.
I think your knowledge of chemistry is weak so I'm going to start with the basics. You have H+ and OH- in solution. If they are equal concentrations, at 10^-7 mmol/L then you have pH of 7. If the hydrogen ion concentration goes up, then you have a lower pH. If it's 10^-6 then your pH is 6. What does a buffer do? It holds onto extra hydrogen ions so that they don't get put into solution. So COO- would become COOH and that H doesn't add to the hydrogen ion concentration. This helps you maintain the pH at a steady level.
So when blood goes through tissues, there's a ton of CO2 diffusing through the endothelial cells and going towards the red blood cells. In the RBCs is carbonic anhydrase that turns CO2 + H2O into H2CO3 which is in equilibrium with H+ and HCO3-. Your blood can carry either H+ or HCO3- but if they get together they will just become h2co3 and go back to CO2 and H2O. So the RBCs hold the H+ and exchange the HCO3- with chloride to bring the bicarbonate into the blood serum. Most of the CO2 travels as bicarb so having a better buffer means that it can hold onto more hydrogens. Some of the CO2 travels attached to hemoglobin or dissolved in solution so the assumptions made before aren't entirely true but are sufficient to explain your question.
I actually had my own question with the question about how osteoblast, osteoclast, and RANK-L levels would be in a patient with osteoporosis? Can someone help me out with that please? I would expect osteoblast activity to be decreased but you need osteoblasts to secrete RANK-L to activate the osteoclasts.
I'm not sure about the cervix thing, I thought it was just always internal iliac.
As far as the other question goes, if you're getting less blood flow into the RV after the closure, then less blood will move into the lungs, and therefore less blood will move into the Left Atrium. This will cause a decreased left atrial pressure relative to before fix. LVP will still increase because it no longer has an extra hole with which it can release all of its blood/pressure.
I'm still confused, shouldn't the exotoxins be inactivated by 1 hour of 350 boiling?Just vomiting. Because they got sick within 4 hours, think of food poisoning via preformed exotoxin. Furuncle/boiil should make you think of a staph-like abscess because coagulase makes it very localized. Staph exotoxin causes vomiting and diarrhea.
I'm still confused, shouldn't the exotoxins be inactivated by 1 hour of 350 boiling?
Got it, thanks!FA2014 on pg. 130 says that S. aureus makes a heat stable enterotoxin that is not destroyed by cooking
The answer is A) Smoking CessationView attachment 183065
Hi all, I have the above question, which is the correct answer? Thanks so much for everybodies' input!
read up on those topics and see bolded parts. Also, what was her age? Absent is more kids.I have a question and need help..!! The question says female with altered consciouness since 6 months. During interview she stops talking n turns her head stiffens her hand n gives a blank look along with reptitive movement of hands. The episode lasts for 30 sec n then she is normal within next 4 to 5 mins. What kind of seizure is this? I felt the answer should be absent but the correct answer was complex partial.. can u plz explain??
Thanks.. the age was 43.. this helped.read up on those topics and see bolded parts. Also, what was her age? Absent is more kids.
Influenza virus strains characterized by differing severity to growth inhibition by weak base ammonium chloride. This questions asks from the given viral gene segments segregates with viral progeny viruses which is resistant to ammonium chloride? The options given are HA, M1/M2, NA, NP, PA. Does anyone know what is ans to this question is n how?
Thanks.. got it.okay this one is sort of interesting from #15... I'll try to break it down best and hopefully it makes sense. Apologize in advance if i sound redundant at all. This question really requires to you look at the info given rather then dwell over the biochemistry/pharm aspect of the question.
AC+ = not inhibited by AC
AC- = inhibited by AC
Higher the Ratio= more virus survives (High AC+ (uninhibited) and a smaller AC- (inhibited), allowing the progeny to survive the replication. )
Lower the ratio= less virus survives
SF- when treated alone with AC yields virus progeny---- aka-- RESISTANT: it is not inhibited by ammonium chloride --- hence [AC+/AC-] ratio =0.8
NY- when treated alone with AC grows poorly---- aka---NONRESISTANT: it is inhibited by ammonium cholride----- hence [AC+/AC-] ratio = 0.005
The question stated that there were two Influ viruses SF and NY that are put through reassortment for 8 generations. What part of the segment is resistant to AC???
Criteria for resistance:
Only the first 5 generation have a AC+/ AC- value that match what we are looking for.
- [AC+/AC-]= close to 1 (which means more have survived after exposure to the AC)
- Whatever the segment, it should have SF part of the genome, since that virus has something that made it resistant in first place
Now look across to the genome segment. The only thing common in the first 5 generation is HA. Also since SF was the one that was resistant.
Answer is HA.
Hope that helps!!
In the question about end plate potential it gave an epp in response to a normal release of acetylcholine. I believe it said a normal epp gave a concentration of 10 micromolar of ach. a mini end plate potential consists of random release of ach that does not amount to more than 1 micromolar, and it said the voltage response was 1mv for every 1 micromolar of ach... if I recall correctly. So then it asked what would happen in the presence of botulism- Botulism would block epp, but would have no effect on mepp (because these are random discahrges of ach) or voltage difference in response to a given amount of ach.
hay i have some questions that i didnt get through
. A 38-year-old man is admitted to the hospital after sustaining a gunshot wound to the abdomen. Broad-spectrum antibiotic therapy is initiated for complications from fecal contamination of the peritoneal cavity. He has been taking warfarin since receiving an artificial heart valve 6 years ago because of endocarditis secondary to intravenous drug use. During the next 6 weeks, the warfarin dosage required to maintain his prothrombin time progressively decreases. Which of the following best explains this finding?
A
) Decreased INR caused by drug-induced hepatotoxicity
B
) Decreased INR caused by hepatitis B infection
C
) Septic shock caused by an anaerobic commensal such as Bifidobacterium species
D
) Septic shock caused by a facultative anaerobe such as Escherichia coli
E
) Vitamin K deficiency caused by bacterial overgrowth in the small intestine
F
) Vitamin K deficiency caused by depletion of the normal gut flora
Cpls help me about this questions
A paper says, "We chose the sample size to have an 80% power of detecting a 15% mean difference with a significance level (two-sided) of 5%." If there really is no difference between the groups overall, which of the following best represents the chance that the study will find a statistically significant difference, and what is this error called?
A
) 0%, Type I error
B
) 0%, Type II error
C
) 5%, Type I error
D
) 5%, Type II error
E
) 15%, Type I error
F
) 15%, Type II error
G
) 20%, Type I error
H
) 20%, Type II error
Apls help me about this questions
19. A 71-year-old woman comes to the physician for a follow-up examination. She has a 30-year history of type 2 diabetes mellitus currently treated with insulin. She is 160 cm (5 ft 3 in) tall and weighs 59 kg (130 lb); BMI is 23 kg/m2. Her blood pressure is 116/78 mm Hg. This patient is most likely to have an endogenous fasting serum insulin concentration (N=5–20 μU/mL) closest to which of the following?
A
) 1 μU/mL
B
) 10 μU/mL
C
) 20 μU/mL
D
) 40 μU/mL
E
) 80 μU/mL
A 3-year-old girl is brought to the physician because of a 1-month history of a lump in her upper neck. Physical examination shows a 2-cm mass in the midline. The mass moves upward with swallowing and protrusion of the tongue. Radionucleotide imaging with technetium 99m pertechnetate shows uptake in the mass. If a biopsy specimen of this mass were obtained, it would most likely show which of the following?
A
) Chief and oxyphil cells
B
) Chondroid matrix
C
) Serous and mucous acini
D
) Taste buds
E
) Thyroid follicles
Hey everyone. I've picked through this thread and haven't seen this Q posted anywhere, so here is a summary since it was a rather long Q:
A previously healthy 27 year-old woman has fever, rash, and progressive confusion. She underwent a sinus operation to remove nasal polyps 2 days ago. PE shows a diffuse rash with erythroderma and hyperemic mucous membranes. Liver edge is palpable. There are a ton of labs run. Pulse is 110. BP is 86/60. Gram-stain shows gram-positive cocci in clusters. The causal organism most likely produced the systemic syndrome by what mechanism?
A) leukocidin mediated lysis of phagocytic cells
B) lipase degradation of lipids
C) Superantigen activation of T-lymphocytes
D) Toxin B mediated cleavage of desmoglein-1
E) a-Toxin mediated depolarization of plasma membranes
- Gram +ive cocci = S. aures
- Pulse and Bp suggest shock
- Recent Nasal polyp operation suggest= another way of hinting Nasal Packing
- Release of TSST-1 (which is a superantigen)
- Activates T-lymphocytes= which release IL-2 and INF- gamma= activate macrophages= which release TNF-alpha, IL- 1= causing shock, fever, hypotension , rash
Hi,Thanks for sharing. I'm taking the exam in a week, but decided against any more NBMEs at this time, so I'm glad to at least get input on the new form. (My confidence will probably be a real factor at the range I'm at, which is why I held off.)
13. OP poisoning. Yeah, atropine, atropine and more atropine. Pralidoxime is for the fasciculations and regeneration of AChE. (Treated a ton of these cases myself, and lost a lot of these pts - common method of suicide for farmers overseas.)
15. Annoying answers choices. I'd say A. Wouldn't E be deferring to someone else? Which is apparently never the right choice.
Pulm edema from ruptured papillary muscle-->mitral regurg47-yo man in the hospital after MI. Pulse ox on 30% O2 shows O2 sat greater than or equal to 95%. 3 hours later, pt develops shortness of breath. Pulse ox now shows O2 sat of 90%. Crackles are heard in the lung base, and grade 2/6 systolic murmur is heard. ABG values on 30% O2 show:
pH: 7.41
PCO2: 36 mmHg
PO2: 60 mmHg
What is the cause of hypoxemia?
a) decreased alveolar ventilation
b) decreased erythrocyte transit time in pulmonary capillaries
c) decreased lymphatic drainage
d) increased permeability of pulmonary capillaries (wrong)
e) increased plasma colloid osmotic pressure
f) increased pulmonary capillary pressure
Any help??
Been a while since I took this, but what I think I remember is in bold. Some questions I don't remember the reasoning for have definitely been answered in this thread already, try searching this thread only for keywords.1) Woman has massive bleeding post pregnancy, Soft uterus and contraction have stopped. Which hormone would be useful for this patient? I put estrogen (wrong). Oxytocin. Contract down the uterus to control bleeding.
2) During a series of normal skeletal muscle twitches, the ATP concentration does not fall appreciably because of which of the following? I put ATP is high but I knew that that was probably wrong. 3 ) creatine phosphate stores replenish ATP immediately
3) A 6-year-old boy, pubic and axillary hair growth. On previous visits, he has been at the 50th percentile for height and weight. Pubic and axillary hair development is Tanner stage 2. enlargement of the testes. If left untreated, which of the following combinations would best describe the likely course of growth in this patient? Gave a bunch of percentiles of one year from now and at adulthood. will grow bigger than peers when young, but be smaller in adulthood due to premature closure of growth plates
4)A 65-year-old woman comes to the physician for a follow-up examination after a DEXA scan showed a decrease in bone density. Was sure I got this one right but why isn't ob's down, oc's up and RANKL down correct? don't remember this question, but RANKL activates osteoclasts.
5) A 67-year-old man is brought to the physician because of a 2-day history of double vision and drooping of his left eyelid. CNIII damage. What happened? I put compression of the superior cervical but that was wrong Pretty sure answered already, not sure what the question is asking
6) A 2-year-old girl is brought to the emergency department 20 minutes after she accidently ingested insecticide. Seeing as pralodoxime is time-sensitive and atropine isn't, why is the immediate step not pralodoxime? also already answered, not sure on the specifics but remember you don't always need pralidoxime, atropine is really the one reversing your sx, so it is more important. atropine also acts more immediately.