- Joined
- Jan 14, 2009
- Messages
- 1,974
- Reaction score
- 2,682
content removed by moderation staff
As above.
Last edited by a moderator:

content removed by moderation staff
Hey guys, surgery is my first rotation - would it be a good idea to read step up to medicine since I haven't had internal med or any other rotation yet? Or should I stick to Uworld/Pestana/just surgery books? Thanks! And sorry for the inappropriate post location, but I think this thread is more frequented than the other ones I've seen...

few questions from the practice shelf...answers and WHY would be greatly appreciated!
1.
46 y/o man with chronic alcoholism comes to ED b/c of 12h history of n/v and midabdominal pain that radiates to the back. HR 120/min, RR 20/min, BP 110/60. Abdominal examination shows tenderness to palpation over the upper quadrants. Bowel sounds are absent. Lab studies show:
Hgb 10.1 g/dL
WBC 24,500
Plt 810,000
Serum
-amylase: 1842 U/L
-albumin: 4.1 g/dL
-Ca: 7.7
Blood glc 248
The most appopropriate next step is IV administration of
a) atropine, b) Calcium gluconate, c) cimetidine, d) imipenem, e) lactated ringer solution
E. This patient has severe pancreatitis. The systemic inflammation causes massive third-spacing of intravascular volume, evidenced here by tachycardia. Replace volume with LR.
2.
36hr after admission to hospital for evaluation of mild-mod diffuse abdominal pain, a 42 y/o woman remains obstipated despite treatment with multiple laxatives. Her last bowel movement was 6d ago. 9 yr history of scleroderma and chronic constipation. 1y history progressive abdominal distention. Current temp is 100.4 *F, HR 110/min, RR 22/min, BP 110/60. Abdomen is distended and tympanitic with diffuse tenderness to deep palpation. There is involuntary guarding and rebound. Hgb is 12 g/dL, and leukocyte count is 14,000. AXR shows dilation of the colon and 12-cm cecum. No distention of small bowel. Which is the most appropriate next step in management?
a) Metoclopramide therapy, b) octreotide therapy, c) colonoscopy, d) sigmoidoscopy, e) laparotomy
E. Bowel obstruction refractory to medical management, now with signs of peritoneal inflammation (guarding, rebound). FYI, the answer is almost always laparotomy when peritoneal signs are present.
3.
1 y/o boy brought to physician because of persistent cough, loose stools, and facial rash for 2 mo. He has had a 1.8 kg weight loss during this period and is currently at the 50th percentile for length and 20th for weight. Appetite and activity remain normal, no hx of fever. Temp is 98.6 *F, HR 100/min, RR 18/min, BP is 80/50 mmHg. Examination shows a malr flush and abdominal distention. CT scan of abdomen shows a small tumor localized to pancreas. The tumor is surgically removed and the patient recovers uneventfully. Which of the following is most likely dx?
a) insulinoma, b) glucagonoma, c) neuroblastoma, d) pancreatic pseudocyst, e) VIP-secreting tumor
E. VIPoma. Giveaway is facial flushing and diarrhea.
4.
67 y/o postal worker comes to physican 1 day after 5m episode of weakness and numbness in R hand while at work. Didn't have any visual problems, headache, or weakness/numbness in LE. Currently asymptomatic. Has smoked 1 PPD x45yrs. Not seen a physician in 40y. HR 85 and irregular, BP is 140/90. Lungs CTAB, pulses palpable. Carotid bruits are heart b/l. Heart sounds are normal except for frequent premature beats. Neurologic examination shows no abnormalities. An ECG shows a NSR with multiple PAC. Which of following is most appopriate next step?
a) Echo, b) carotid duplex U/S, c) heparin therapy, d) TPA therapy, e) warfarin therapy
Hmm, I would say B. I think the afib is a distractor. Patient had a TIA, likely carotid stenosis.
5.
12h after undergoing drainage of pancreatic abscess, 52 yoM with alcholism becomes bradycardic and hypoxic and requires intubation and mechanical ventilation. Weighs 70kg. Ventilator is set at an FiO2 of 100%, tidal volume of 1000 mL, and positive end-expiratory pressure of 2.5cm H2O. Arterial blood gas analysis shows:
pH 7.36
PCO2 40 mmHg
PO2 48 mmHg
Which is most appropriate next step?
a) begin IV acetazolamide therapy, b) begin IV furosemide therapy, c) begin IV heparin therapy, d) begin IV sodium bicarb, e) begin IC urokinase, f) Decrease FiO2, g) decrease tidal volume, h) increase PEEP, i) increase tidal volume
H. ABG shows patient is hypoxemic. 2 ways to increase PO2 are increasing FiO2 (already at 100%) and increasing PEEP. Peep of 2.5 is pretty low, so you've got some room to maneuver. As an aside, tidal volume of 1000 for 70kg man is way high, especially for likely ARDS (which you usually treat with low tidal volume/increased PEEP ventilation). But monkeying with tidal volume will not correct the patient's hypoxemia.
Thanks so much.As above.
Thanks so much.
About the afib one...I understand why you'd Carotid DUS him, but...
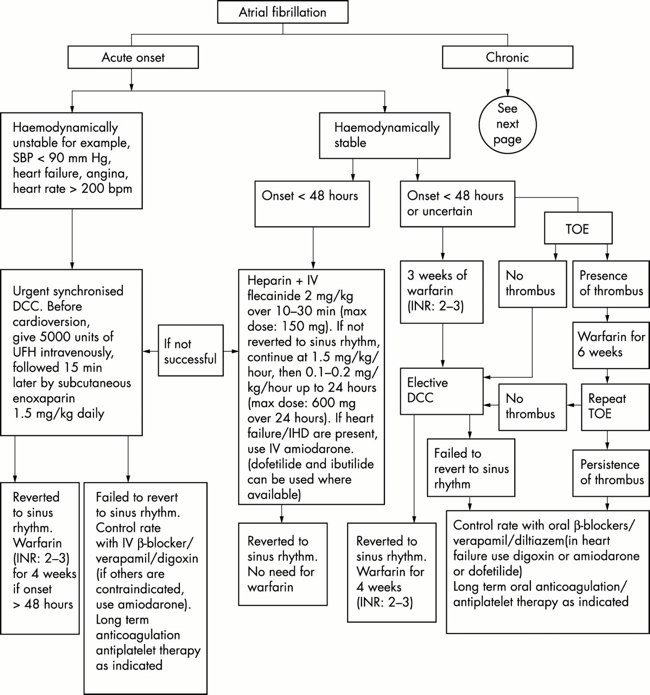
^why would this algorithm not be indicated and medical therapy prescribed?
Definitely read step up to medicine. Take to heart when people say surgery is mostly internal medicine, as far as the shelf exams go. I learned that part the hard way.
My approach would be to read pestana and get a feel for the systematic approach to the questions (i.e. pt presents with ____, what is the most appropriate/what to do next/likely diagnosis/etc). This will help with timing on the test and make pulling out the important points in a question stem second nature. It will also give you a chance to step back and look at the whole patient to see what points they are trying to connect for you. There is a lot of extraneous material there to throw you off, so the faster you get at seeing the patterns of pertinent info (age, time course, labs, imaging, etc.), the better off you'll be. It just takes practice, persistence, and patience.
As you do UWorld/Kaplan/pretest/whatever, read up on things you aren't familiar with in step up/essentials of surgery. Supplement with case files for a change of pace to get the clinical feel of how to flow through algorithms.
And don't forget the immortal words of Goljan, "the more you read, the more you know. It's as simple as that."
Thanks so much.
About the afib one...I understand why you'd Carotid DUS him, but...
^why would this algorithm not be indicated and medical therapy prescribed?
In addition to what VT said, patient in the vignette doesn't have Afib, or at least didn't when they did the EKG. NSR and PACs is not afib. They just wrote the distractors in a mean way to sucker people down that road. Really they handed it over on a silver platter: TIA, no afib, +carotid bruits = duplex and probably a CEA soon to follow.
This post is hilarious.Well, shoot, I got a 65 raw. Did Pestana's twice, Uworld surg once+GI+Fluids and electrolytes, NMS cases once. It was my first rotation. Whatever, I f***in hated surgery anyways. Surgeons always act way smarter than everyone else, when everyone knows they're not. Good riddance.
This post is hilarious.
"ugh they think they're so smart"
Gets 65 on their exam.
Any idea how many questions you need to get right to pass? I believe my school requires a score of "70"...what percentage does that equate to usually?
I'm not sure I've ever seen that data clearly stated. There's a lot of confusion among students regarding how shelves are scored as many conflate "raw" and "scaled" scores as well as "percentiles" and "percent correct."
My guess is you can miss quite a few. I'm usually good at calculating this sort of thing, but surgery was my first shelf and I felt very ambiguous about a LOT of questions. Was shocked to have scored so well on it; part of me still thinks there was an error in my favor but I'm not digging into it!
If I had to guess, I'd say 60 +/- 5 out of 100 correct probably equates to a scaled score of 70. I looked for an authoritative source last year but never did find one.
Raw score means # of correct answers out of 100 right??
No reading?80% --- not sure if percentile, raw, or scaled --- school did not specify
Just did uworld surgery and about 30% of pretest.
Sorry I forgot to mention I read pestana 1x and did most of the questions. If I had more time I would've liked to reread it and finish the questions. I also tried to watch the onlinemeded videos but I got bored after two or three of them.No reading?
Completely agree. Wish I would have found it before the last 2 weeks.Case files surgery is the best book for surgery clerkship
kidney stoneFor 4 hours, a 55 year old male has acute intermittent pain that begins in right flank and radiates to right testicle. Most likely finding on Urinalysis? Why is the answer "Microscopic hematuria (RBC 30/hpf in sediment)" please explain