- Joined
- Aug 17, 2012
- Messages
- 2,283
- Reaction score
- 2,920
- Points
- 5,771
Advertisement - Members don't see this ad
Last edited:

Ecmo
Yeah, I guess that’s what I’m saying with fem fem bypass. Post op trach.
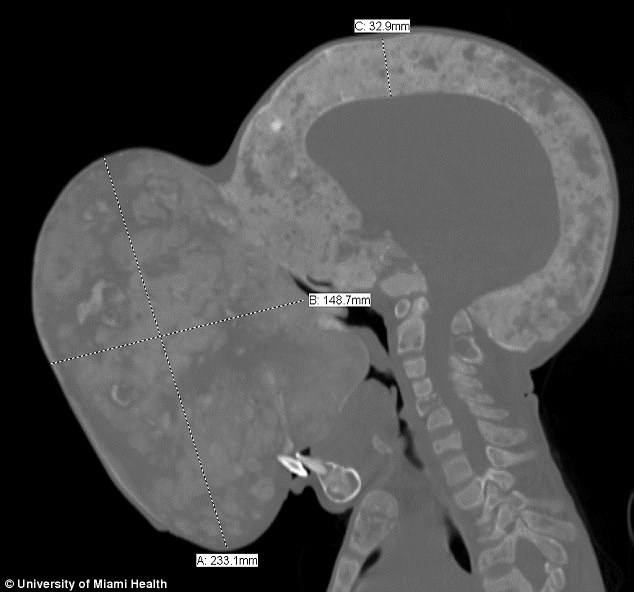
I'm curious if anybody on here has had experience with something like that. ECMO as the plan for a bad airway.I’m thinking fem-fem bypass from the picture, but maybe there is access for sedated trach.
I'm curious if anybody on here has had experience with something like that. ECMO as the plan for a bad airway.
At the children's hospital where I did residency they had a young teen with an enormous mediastinal mass. They did an SAB followed by awake venous groin canulation and initiation of V-V bypass.
Med mass? You mean fem-fem V-A bypass, right?
why va? This is airway obstruction without heart failure? Surely vv would work or am I missing something?Med mass? You mean fem-fem V-A bypass, right?
why va? This is airway obstruction without heart failure? Surely vv would work or am I missing something?
So for the bypass advocates - you go on bypass, then off to sleep, then secure airway, then come off bypass and give protamine?
I believe that is a skin fold.What's wrong with the back of his neck? Why is there a little black space there
Not in that study but I think he should be able to extend the cervical spine just fine. Or at least enough. I think one could slip an LMA in there and call it a day 😉Shiet that’s not a lot of space between the mandible and the manubrium.
I saw that too. WTF?The skull thickness is impressive.
It’s not midlineThe skull thickness is impressive.
Yeah I think that head is both turned and tilted. The cspine is mostly centered but that's about it.It’s not midline
Guys, that’s his true skull thickness. If you read up on the illness, these patients bones get eaten up by fibrous tissue and they end up developing a lot of skeletal deformities.
The mass on his face stems from facial bones being replaced by fibrous tissue. It can affect one part of their body or many parts of it.
Read up guys. Can’t remember the name for the disease right this minute though.
Guys, that’s his true skull thickness. If you read up on the illness, these patients bones get eaten up by fibrous tissue and they end up developing a lot of skeletal deformities.
The mass on his face stems from facial bones being replaced by fibrous tissue. It can affect one part of their body or many parts of it.
Read up guys. Can’t remember the name for the disease right this minute though.
I don’t know what this child’s pathology is, and you are sadly probably right ... but whether this slice is midline is important ... this might be a slice taken to demonstrate maximal dimension of the mass to be excised.Guys, that’s his true skull thickness. If you read up on the illness, these patients bones get eaten up by fibrous tissue and they end up developing a lot of skeletal deformities.
The mass on his face stems from facial bones being replaced by fibrous tissue. It can affect one part of their body or many parts of it.
Read up guys. Can’t remember the name for the disease right this minute though.
ok chill - you frighten me with your caps lock. you are right about the pathology.Jobsfan,
I am NOT PROBABLY RIGHT. I am right. And yes, I know about the difference in appearance depending on where the slices are taken.
The condition is actually in the first linked article called polyostotic fibrous dysplasia. Look up X-rays of this condition.
Look at the bone density of the skull. You see the thinned bone/hollowed out areas that should appear completely uniform but aren't? As in should appear completely white/gray like in your example? Thats's because bone has been replaced and thickened by fibrous tissue.
That’s what she said...that is some major disease, but yea look at that ridiculous bone density to go with the thickness. wow
Looks like the kid survived whatever surgery they did / attempted.
What this 14-year-old thought was a pimple turned into an 8-pound tumor
However, post-op respiratory / renal complications lead to his death.
Cuban boy with giant tumor dies after surgery