
drewdog1973
Full Member
- Joined
- Nov 26, 2020
- Messages
- 299
- Reaction score
- 622
Though I’m a SIB fan, this is true. Acute toxicity is going to increase with higher absolute dose. this is the problem with 0529 for Anal when you give 45 / 30 to elective / low risk areas that previously were treated to 30.6/17 fx ... but I love SIB in general. Just finding the magic doses... I like 54/33..How about 30 Gy... 0% Gr3 or greater(!) toxicity rate. Regardless, 56/35 to elective areas is tougher on patients IMHO versus 50/25 (or 40/20), either of which can only be rationally achieved by staging (ie "two-scan planning," or more) the dosing.
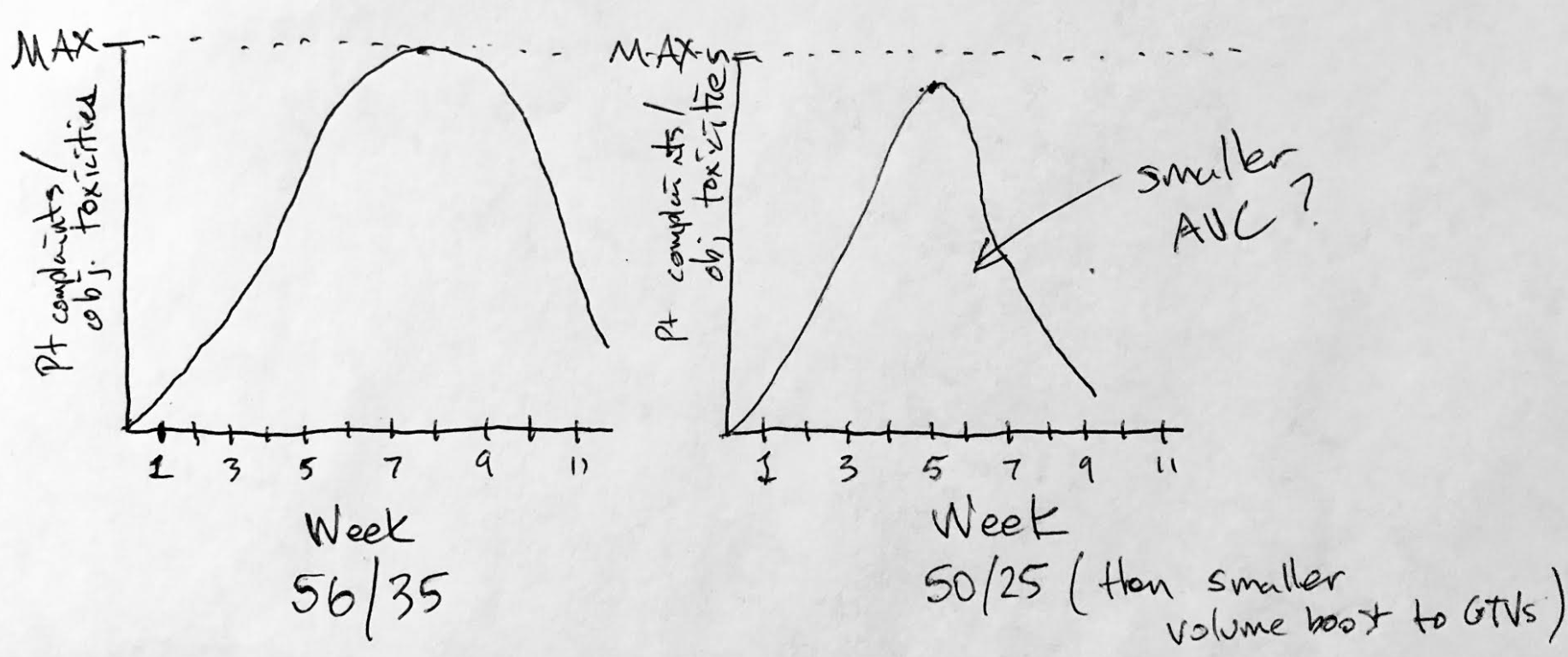
") It's (supposed to be) a rad bio truism that total dose governs acute toxicity to a much larger degree than fraction size does.
It's (supposed to be) a rad bio truism that total dose governs acute toxicity to a much larger degree than fraction size does.