How many of you prescribe opioids to both a husband and wife at the same time? If so, is it a one-off occurrence or do you regularly prescribe opioids to patients who live within the same household? Why or why not?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Question about Opioid Prescribing Practices
- Thread starter potcake76
- Start date

- Joined
- Oct 7, 2011
- Messages
- 16,809
- Reaction score
- 7,287
no, not a regular occurrence.
i have one inherited couple in which both husband and wife were started by someone else. one member with time stopped using. the other still does use oxycodone.
i currently do have roughly 10 or so husband wife situations. including the above, there are 2 other couples in which one member uses tramadol and the other is not on opioids.
it is an individual assessment of the patient to see if opioid medication is appropriate.
i have one inherited couple in which both husband and wife were started by someone else. one member with time stopped using. the other still does use oxycodone.
i currently do have roughly 10 or so husband wife situations. including the above, there are 2 other couples in which one member uses tramadol and the other is not on opioids.
it is an individual assessment of the patient to see if opioid medication is appropriate.
I inherited a few husband and wife couples, both on opioids. If I feel it is indicated I’ll continue the regimen, but will make sure they’re on different opioids and track their UDS to make sure they’re still using appropriately and not using each other’s prescriptions
- Joined
- Apr 6, 2007
- Messages
- 2,162
- Reaction score
- 1,155
ive seen spouses use their SO to attempt to get opioids once they were flagged for aberrancy... UDS, etc
had one wife correct her husband re the medication he needed while they were both in my clinic room
had one wife correct her husband re the medication he needed while they were both in my clinic room
- Joined
- Oct 23, 2005
- Messages
- 8,279
- Reaction score
- 6,025
Definitely a bad dynamic with two spouses on opioids
- Joined
- May 30, 2005
- Messages
- 23,349
- Reaction score
- 14,996
It is a common thing.
When one messes up, both pay the price.
When one messes up, both pay the price.
- Joined
- Nov 16, 2005
- Messages
- 1,469
- Reaction score
- 1,141
I've had 3 or 4 of these couples in the past couple of years. None are currently being treated by me as a couple anymore. One the husband said he couldn't afford butrans anymore, told him that was his only option, he's no longer my patient, though the wife still comes to me. One the husband was positive for THC x2, fired him and wife quit. Another the husband went on medicaid but wife kept her work insurance. (looks like it's always the husbands who are the problem...)
I have one father/daughter duo who live together, and are very compliant with their low dose opioids
When I'm reviewing referrals, I definitely consider husband/wife opioid team to be strike 1
I have one father/daughter duo who live together, and are very compliant with their low dose opioids
When I'm reviewing referrals, I definitely consider husband/wife opioid team to be strike 1
- Joined
- Oct 23, 2005
- Messages
- 8,279
- Reaction score
- 6,025
Good job holding holding the line on butrans.I've had 3 or 4 of these couples in the past couple of years. None are currently being treated by me as a couple anymore. One the husband said he couldn't afford butrans anymore, told him that was his only option, he's no longer my patient, though the wife still comes to me. One the husband was positive for THC x2, fired him and wife quit. Another the husband went on medicaid but wife kept her work insurance. (looks like it's always the husbands who are the problem...)
I have one father/daughter duo who live together, and are very compliant with their low dose opioids
When I'm reviewing referrals, I definitely consider husband/wife opioid team to be strike 1
Now that it is generic, with goodrx card it can be obtained for $60. Everyone can afford that.
And to ducttape. Everyone can afford that. Or they can get a part time job if not. And everyone, I mean everyone can find work for one day a month if properly motivated, and not coddled by the government.
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
Which jobs are offering 1 day of work a month that a disabled or elderly person can do? Most prn work is day laborer, in my area at leastGood job holding holding the line on butrans.
Now that it is generic, with goodrx card it can be obtained for $60. Everyone can afford that.
And to ducttape. Everyone can afford that. Or they can get a part time job if not. And everyone, I mean everyone can find work for one day a month if properly motivated, and not coddled by the government.
- Joined
- Jun 10, 2011
- Messages
- 424
- Reaction score
- 272
What pharmacy has it for $60? Lowest I see by me is $90 at Kroger.Good job holding holding the line on butrans.
Now that it is generic, with goodrx card it can be obtained for $60. Everyone can afford that.
And to ducttape. Everyone can afford that. Or they can get a part time job if not. And everyone, I mean everyone can find work for one day a month if properly motivated, and not coddled by the government.
Edit: Nvm. GoodRx defaulted to 10mcg patches. 5mcg start at $54 near me. Didn't know it had dropped that low, really glad to hear this.
- Joined
- Oct 23, 2005
- Messages
- 8,279
- Reaction score
- 6,025
1-Walmart greeter.Which jobs are offering 1 day of work a month that a disabled or elderly person can do? Most prn work is day laborer, in my area at least
2-All kinds of low impact low level part time office jobs.
(Particularly With any dental/medical office)
3- many other low impact part time jobs out there, particularly in todays economy.
I have hundreds of Medicare age patients in the Rockies who still work part time. Not because they have to, but because they find meaning in getting off the couch and doing something.
My ortho partner have several ranchers out here who opted for a 1-2 segment finger amputation instead of a repair because it would take them away too long from work on their ranch.
Just a few examples of why red state conservatives don’t believe in handouts to lazy people who live in blue areas near the coasts/big cities who want to act like helpless infants demanding the government take care of their every need (like infants) instead of getting off their asses to do something.
Last edited:
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
Bedrock, does your clinic want to hire a disabled or elderly person for a few hours a week? I know mine doesn’t.1-Walmart greeter.
2-All kinds of low impact low level part time office jobs.
(Particularly With any dental/medical office)
3- many other low impact part time jobs out there, particularly in todays economy.
I have hundreds of Medicare age patients in the Rockies who still work part time. Not because they have to, but because they find meaning in getting off the couch and doing something.
My ortho partner have several ranchers out here who opted for a 1-2 segment finger amputation instead of a repair because it would take them away too long from work on their ranch.
Just a few examples of why red state conservatives don’t believe in handouts to lazy people who live in blue areas near the coasts/big cities who want to act like helpless infants demanding the government take care of their every need (like infants) instead of getting off their asses to do something.
I can tell you, living in the red part of Texas, that wanting to get on disability, stop working, eat pain pills, get sedated for simple shots and cheat on workers compensation is not related to political affiliation. The only difference is somehow my 40-some disabled proud Texan who can still ride a motorcycle and go hunting still thinks he’s better than me.
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
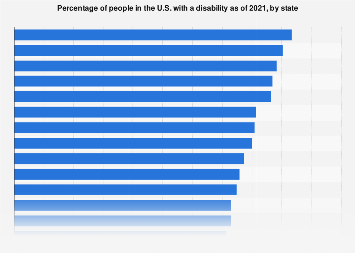
Disability rates by state U.S.| Statista
The state with the highest disability rate is West Virginia. New Jersey has the lowest disability rate with 10.8 percent.
 www.statista.com
www.statista.com
- Joined
- Jul 27, 2017
- Messages
- 191
- Reaction score
- 271
1-Walmart greeter.
2-All kinds of low impact low level part time office jobs.
(Particularly With any dental/medical office)
3- many other low impact part time jobs out there, particularly in todays economy.
I have hundreds of Medicare age patients in the Rockies who still work part time. Not because they have to, but because they find meaning in getting off the couch and doing something.
My ortho partner have several ranchers out here who opted for a 1-2 segment finger amputation instead of a repair because it would take them away too long from work on their ranch.
Just a few examples of why red state conservatives don’t believe in handouts to lazy people who live in blue areas near the coasts/big cities who want to act like helpless infants demanding the government take care of their every need (like infants) instead of getting off their asses to do something.
The hundreds of Medicare patients I see in deep red rural Texas aren’t paying 60 bucks for a Butrans patch. They are some of the laziest/entitled people around. Oh and the same goes for the Medicare patients I see in the deep blue city nearby. Welcome to America.
D
deleted875186
Not a political issue, it’s a socioeconomic one. Economically depressed areas have a higher disabled population, which also tend to be more often republican states. The comment above about entitled handouts to blue states is absurd, but I have no doubt this is actually what people in the republican states think.Disability rates by state U.S.| Statista
The state with the highest disability rate is West Virginia. New Jersey has the lowest disability rate with 10.8 percent.
View attachment 369667
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
Interestingly, the lowest disability states were Utah, New Jersey, and California.Not a political issue, it’s a socioeconomic one. Economically depressed areas have a higher disabled population, which also tend to be more often republican states. The comment above about entitled handouts to blue states is absurd, but I have no doubt this is actually what people in the republican states think.
- Joined
- Oct 23, 2005
- Messages
- 8,279
- Reaction score
- 6,025
Bedrock, does your clinic want to hire a disabled or elderly person for a few hours a week? I know mine doesn’t.
I can tell you, living in the red part of Texas, that wanting to get on disability, stop working, eat pain pills, get sedated for simple shots and cheat on workers compensation is not related to political affiliation. The only difference is somehow my 40-some disabled proud Texan who can still ride a motorcycle and go hunting still thinks he’s better than me.
The hundreds of Medicare patients I see in deep red rural Texas aren’t paying 60 bucks for a Butrans patch. They are some of the laziest/entitled people around. Oh and the same goes for the Medicare patients I see in the deep blue city nearby. Welcome to America.
Disability rates by state U.S.| Statista
The state with the highest disability rate is West Virginia. New Jersey has the lowest disability rate with 10.8 percent.
View attachment 369667
I don't think any of you read the fine print. This is not a list of patient on SSI, it is a list of patients with any disability at all, including just vision or hearing impairment.
A more accurate map, might be one for medicaid. Notice that that outside of appalachia, the states with the most people getting medicaid are...........blue states! And in the mountain west, its interesting to note that blue state of colorado and purple state of Montana had many more people on medicaid, than the red states next door..........hmm??????????
Percentage of Population Enrolled in Medicaid or CHIP by State | Medicaid
That said, there are still plenty of lazy POS out there in any state who are happy to live off the government and our taxes. Why??
Because the democrats coddle them and give them free stuff, either because the dems are ignorant of the human condition or just to buy votes, I'm not sure which.
My pain point is that if someone really needs butrans they can find a way to pay $60 a month.
I do think that all bup products should be covered with a modest copay by all US insurances, but until they are, I will not let a lazy person give me any grief about requiring they work a little, or maybe read instead of watching cable all day.
Last edited:
- Joined
- Oct 23, 2005
- Messages
- 8,279
- Reaction score
- 6,025
Bedrock, does your clinic want to hire a disabled or elderly person for a few hours a week? I know mine doesn’t.
I can tell you, living in the red part of Texas, that wanting to get on disability, stop working, eat pain pills, get sedated for simple shots and cheat on workers compensation is not related to political affiliation. The only difference is somehow my 40-some disabled proud Texan who can still ride a motorcycle and go hunting still thinks he’s better than me.
The hundreds of Medicare patients I see in deep red rural Texas aren’t paying 60 bucks for a Butrans patch. They are some of the laziest/entitled people around. Oh and the same goes for the Medicare patients I see in the deep blue city nearby. Welcome to America.
If they fail PT, procedures, tramadol/gabapentin and think its outrageous to have to pay $60 for butrans, then I show them the door. I don't have time for lazy entitled slugs. Hard to be certain which medicare patients actually worked a full life vs ones who got on SSI at 40 and are really just old medicaid patients, now on medicare.
To agast, I'm certainly not saying there are not plenty of lazy entitled people who vote republican in Texas, but the majority of SSI/medicaid in the entire USA definitely vote democrat.
And to agast, many medical practices including all of mine, are happy to hire college students/seniors to do basic filing etc, 1-2 days a week because the practice doesn't have to pay benefits. Two half time or four quarter time employees are much cheaper than two full time employees.
The trend in business is to hire as many part-time employees as possible so you don't have to pay benefits.
I guess your practice isn't very business savvy.
Last edited:
- Joined
- Dec 13, 2005
- Messages
- 6,794
- Reaction score
- 5,500
“I’m just worn out from working all my life.”
Scans medical record. Birth year: 1986. Story checks out. Norco RX signed and sent.
Scans medical record. Birth year: 1986. Story checks out. Norco RX signed and sent.
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
ok, since you hire so many part-time employees - how many of them are disabled or elderly and needing the money to afford their prescription drugs? That was your original proposal. Hiring a bunch of college kids isn’t a revolutionary business plan. I prefer not to hire people over a certain age because they struggle with learning the EMR. I watched someone type with two fingers, it was physically painful.And to agast, many medical practices including all of mine, are happy to hire college students/seniors to do basic filing etc, 1-2 days a week because the practice doesn't have to pay benefits. Two half time or four quarter time employees are much cheaper than two full time employees.
The trend in business is to hire as many part-time employees as possible so you don't have to pay benefits.
I guess your practice isn't very business savvy.
- Joined
- Jan 2, 2016
- Messages
- 2,846
- Reaction score
- 2,954
You’re the first person I know who moved from CA to CO and made CO less socialist. Thanks!1-Walmart greeter.
2-All kinds of low impact low level part time office jobs.
(Particularly With any dental/medical office)
3- many other low impact part time jobs out there, particularly in todays economy.
I have hundreds of Medicare age patients in the Rockies who still work part time. Not because they have to, but because they find meaning in getting off the couch and doing something.
My ortho partner have several ranchers out here who opted for a 1-2 segment finger amputation instead of a repair because it would take them away too long from work on their ranch.
Just a few examples of why red state conservatives don’t believe in handouts to lazy people who live in blue areas near the coasts/big cities who want to act like helpless infants demanding the government take care of their every need (like infants) instead of getting off their asses to do something.
- Joined
- Oct 23, 2005
- Messages
- 8,279
- Reaction score
- 6,025
😂😂😂. I grew up in the mountains of Idaho, where you earn what you earn and nothing is handed to you.You’re the first person I know who moved from CA to CO and made CO less socialist. Thanks!
5 years in LA didn’t corrupt my perspective on meritocracy.
I moved to the direct political center after my time training in NYC and Boston 15-20 years ago.
However, I’m likely considered center right instead of direct center at this point, because the democrats have gone so far crazy left in the past decade.
Last edited:
- Joined
- Oct 7, 2011
- Messages
- 16,809
- Reaction score
- 7,287
i beg to differ.Good job holding holding the line on butrans.
Now that it is generic, with goodrx card it can be obtained for $60. Everyone can afford that.
And to ducttape. Everyone can afford that. Or they can get a part time job if not. And everyone, I mean everyone can find work for one day a month if properly motivated, and not coddled by the government.
you must not take care of any LOL or elderly males that struggle to get to your office, have no transportation, and are on government fixed incomes that barely cover rent.
your data is skewed because 10 states have still not expanded Medicaid - Wyoming, Kansas, Texas, Wisconsin, Tennessee, Mississippi, Alabama, Georgia, South Carolina and Florida. that essentially includes all of the south except Louisiana.I don't think any of you read the fine print. This is not a list of patient on SSI, it is a list of patients with any disability at all, including just vision or hearing impairment.
A more accurate map, might be one for medicaid. Notice that that outside of appalachia, the states with the most people getting medicaid are...........blue states! And in the mountain west, its interesting to note that blue state of colorado and purple state of Montana had many more people on medicaid, than the red states next door..........hmm??????????
Percentage of Population Enrolled in Medicaid or CHIP by State | Medicaid
That said, there are still plenty of lazy POS out there in any state who are happy to live off the government and our taxes. Why??
Because the democrats coddle them and give them free stuff, either because the dems are ignorant of the human condition or just to buy votes, I'm not sure which.
My pain point is that if someone really needs butrans they can find a way to pay $60 a month.
I do think that all bup products should be covered with a modest copay by all US insurances, but until they are, I will not let a lazy person give me any grief about requiring they work a little, or maybe read instead of watching cable all day.
the uninsured rates in these states apparently is double what it is than in insured states.

How Many Uninsured Are in the Coverage Gap and How Many Could be Eligible if All States Adopted the Medicaid Expansion? | KFF
This analysis estimates that 1.4 million uninsured individuals in the ten states without Medicaid expansion, including many working adults, people of color, and those with disabilities, remain in the "coverage gap," ineligible for Medicaid or for tax credits that would make coverage through the...
 www.kff.org
www.kff.org
- Joined
- Oct 21, 2008
- Messages
- 2,859
- Reaction score
- 3,429
Yup. I’ve worked in three states, and it’s not much surprise that the state where I saw the most people on disability (Alabama) was also the reddest.Not a political issue, it’s a socioeconomic one. Economically depressed areas have a higher disabled population, which also tend to be more often republican states. The comment above about entitled handouts to blue states is absurd, but I have no doubt this is actually what people in the republican states think.
D
deleted885753
You must be practicing in Beverley hills or something. Vast majority of folks in my corner would scoff at $20 copay for their meds, let alone paying $60/month..
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
I see doctors on Facebook groups complaining all the time how much things cost. I can’t imagine it feels much better when you’re on a fixed income $800/month. A senior living community apartment starts at like $3500/month and that’s just for access to meals and amenities.
- Joined
- Nov 16, 2005
- Messages
- 1,469
- Reaction score
- 1,141
I mean, he was complaining in another thread about his 30% medicare population...i beg to differ.
you must not take care of any LOL or elderly males that struggle to get to your office, have no transportation, and are on government fixed incomes that barely cover rent.
- Joined
- Nov 16, 2005
- Messages
- 1,469
- Reaction score
- 1,141
Now let's start talking about PT copays. I had a pt this morning telling me they were asking $95 a visit, and wanting her to go twice a week. I could pay that, but I wouldn't want to. That's impossible money to lots of people on fixed incomesYou must be practicing in Beverley hills or something. Vast majority of folks in my corner would scoff at $20 copay for their meds, let alone paying $60/month..
- Joined
- Oct 7, 2011
- Messages
- 16,809
- Reaction score
- 7,287
in more detail...
yes, the lower income people are more likely to vote democrat. why is that a surprise? the republican party platform disincentives and does not benefit those of lower income. in fact, one can make the cogent point that MAGA policies do not benefit the middle class.
as a side not, interestingly, when discussing medicaid expansion, based on this survey, the people most likely to favor medicaid expansion are those with college education, not with differences in socioeconomic status or race...

 insight.kellogg.northwestern.edu
insight.kellogg.northwestern.edu
yes, the lower income people are more likely to vote democrat. why is that a surprise? the republican party platform disincentives and does not benefit those of lower income. in fact, one can make the cogent point that MAGA policies do not benefit the middle class.
as a side not, interestingly, when discussing medicaid expansion, based on this survey, the people most likely to favor medicaid expansion are those with college education, not with differences in socioeconomic status or race...
Which Voters Want to Expand Medicaid? Maybe Not the Ones You Think
4-year degree-holders tend to be big supporters—even though they are personally unlikely to benefit.
insight.kellogg.northwestern.edu
- Joined
- Jan 2, 2016
- Messages
- 2,846
- Reaction score
- 2,954
This has little to do with practice locale. Many of my patients complain about a copay, but gladly cough up $300/month to have an NP put a pellet in their @$$ to provide "lifesaving hormones."You must be practicing in Beverley hills or something. Vast majority of folks in my corner would scoff at $20 copay for their meds, let alone paying $60/month..
Ducttape's patients probably complain about a copay that costs a fraction of a carton of cigarettes.
- Joined
- Dec 12, 2006
- Messages
- 3,107
- Reaction score
- 3,679
“I’m just worn out from working all my life.”
Scans medical record. Birth year: 1986. Story checks out. Norco RX signed and sent.
- Joined
- Oct 7, 2011
- Messages
- 16,809
- Reaction score
- 7,287
yet you wont believe how many patients i have had who say they stopped smoking because they couldnt afford their cigarettes.This has little to do with practice locale. Many of my patients complain about a copay, but gladly cough up $300/month to have an NP put a pellet in their @$$ to provide "lifesaving hormones."
Ducttape's patients probably complain about a copay that costs a fraction of a carton of cigarettes.
- Joined
- Apr 13, 2016
- Messages
- 3,477
- Reaction score
- 3,596
The homeless guy I saw today still manages to scrape together funds for them. Too bad too because he’s pretty myelopathic and needs surgery. Hopefully he can quit before then.yet you wont believe how many patients i have had who say they stopped smoking because they couldnt afford their cigarettes.
- Joined
- Dec 30, 2014
- Messages
- 68
- Reaction score
- 40
Of course I read a thread like this and have an issue a few days later.
Inherited husband and wife couple in mid 60s. Have been seen for a decade (possibly even longer, EMR only goes so far back) in our clinic and essentially on opiates since their first visit. Wife on 10mg hydrocodone QID PRN. Doing poorly. Newish rotator cuff tear. Can't afford PT. Injection by ortho only helped for a short time. No plans for surgery apparently. Left-sided low back pain with a referral pattern down left thigh. Not conistent with radicular pain. Not big on injections since nothing has worked. Wonder what I am doing here.
Husband on oxycodone 10mg TID PRN. Pain seemingly consistent with LLE sciatica, but who knows since his last MRI was from 2013. Can't afford another MRI.
Roomed these patients separately the first time I saw them, but my schedule was overbooked so I saw them together to save time. Probably bad idea in general, but I did get to see a useful dynamic.
Interview wife as above. Like pulling teeth. Interview husband. Husband says he is doing well. Wife chimes in and says that he is too scared to ask for more or a higher dose. Give spiel that I am not increasing these doses. Red flag. Her UDS is positive for oxycodone. Still awaiting confirmation. Going to bring them in on short notice for UDS and pill count if confirmation positive. Best case scenario they both get placed on Butrans.
I could go on and on about this doctor, but neither the time nor place.
Inherited husband and wife couple in mid 60s. Have been seen for a decade (possibly even longer, EMR only goes so far back) in our clinic and essentially on opiates since their first visit. Wife on 10mg hydrocodone QID PRN. Doing poorly. Newish rotator cuff tear. Can't afford PT. Injection by ortho only helped for a short time. No plans for surgery apparently. Left-sided low back pain with a referral pattern down left thigh. Not conistent with radicular pain. Not big on injections since nothing has worked. Wonder what I am doing here.
Husband on oxycodone 10mg TID PRN. Pain seemingly consistent with LLE sciatica, but who knows since his last MRI was from 2013. Can't afford another MRI.
Roomed these patients separately the first time I saw them, but my schedule was overbooked so I saw them together to save time. Probably bad idea in general, but I did get to see a useful dynamic.
Interview wife as above. Like pulling teeth. Interview husband. Husband says he is doing well. Wife chimes in and says that he is too scared to ask for more or a higher dose. Give spiel that I am not increasing these doses. Red flag. Her UDS is positive for oxycodone. Still awaiting confirmation. Going to bring them in on short notice for UDS and pill count if confirmation positive. Best case scenario they both get placed on Butrans.
I could go on and on about this doctor, but neither the time nor place.
- Joined
- Oct 23, 2005
- Messages
- 8,279
- Reaction score
- 6,025
Best case scenario is they leave and never come back.
Nothing in your description justifies oxycodone for either patient.
they bring up increased doses, that is your cue to say the oxycodone isn’t working.
Then you tell them the only controlled substance option they have is butrans.
They will likely discharge themselves. If not, butrans is a much better option for these two.
Nothing in your description justifies oxycodone for either patient.
they bring up increased doses, that is your cue to say the oxycodone isn’t working.
Then you tell them the only controlled substance option they have is butrans.
They will likely discharge themselves. If not, butrans is a much better option for these two.
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
My friend, you have been gifted a beautiful opportunity. You get a 2-for-1 fire sale. You document that the wife insisted you prescribe her husband more oxycodone. Wife then tests positive for oxycodone not prescribed to her. You don't have to prove it came from the husband, the fact is he was sitting there fully complicit and went along with her lying to the pain physician. Once trust has been broken, there cannot be a therapeutic relationship. I wouldn't bother with the pill count, because if he somehow passed would you plan on keeping him as a patient?Of course I read a thread like this and have an issue a few days later.
Inherited husband and wife couple in mid 60s. Have been seen for a decade (possibly even longer, EMR only goes so far back) in our clinic and essentially on opiates since their first visit. Wife on 10mg hydrocodone QID PRN. Doing poorly. Newish rotator cuff tear. Can't afford PT. Injection by ortho only helped for a short time. No plans for surgery apparently. Left-sided low back pain with a referral pattern down left thigh. Not conistent with radicular pain. Not big on injections since nothing has worked. Wonder what I am doing here.
Husband on oxycodone 10mg TID PRN. Pain seemingly consistent with LLE sciatica, but who knows since his last MRI was from 2013. Can't afford another MRI.
Roomed these patients separately the first time I saw them, but my schedule was overbooked so I saw them together to save time. Probably bad idea in general, but I did get to see a useful dynamic.
Interview wife as above. Like pulling teeth. Interview husband. Husband says he is doing well. Wife chimes in and says that he is too scared to ask for more or a higher dose. Give spiel that I am not increasing these doses. Red flag. Her UDS is positive for oxycodone. Still awaiting confirmation. Going to bring them in on short notice for UDS and pill count if confirmation positive. Best case scenario they both get placed on Butrans.
I could go on and on about this doctor, but neither the time nor place.
- Joined
- Oct 7, 2011
- Messages
- 16,809
- Reaction score
- 7,287
i would tell them that you cannot prescribe to either. the wife is positive for a different substance than what she is taking. misuse, borders on addiction criteria.
the husband may be appropriate, but he has demonstrated that he cannot keep his medications stored safely.
and this is probably why the wife is requesting a higher dose for the husband - so she can take his meds along with hers.
they will say that the specimens were messed up, and your lab screwed up the labelling. be prepared to defend against this accusation, becuase then they will try to go down the rabbit hole of reordering their urines to give you time to change your mind.
tell them that your office cannot, but you cannot say so for other pain clinics.
you are more than happy to evaluate them further with regards to non-opioid to see if anything has changed.
i personally would not prescribe a tapering script.
the husband may be appropriate, but he has demonstrated that he cannot keep his medications stored safely.
and this is probably why the wife is requesting a higher dose for the husband - so she can take his meds along with hers.
they will say that the specimens were messed up, and your lab screwed up the labelling. be prepared to defend against this accusation, becuase then they will try to go down the rabbit hole of reordering their urines to give you time to change your mind.
tell them that your office cannot, but you cannot say so for other pain clinics.
you are more than happy to evaluate them further with regards to non-opioid to see if anything has changed.
i personally would not prescribe a tapering script.
- Joined
- Jun 16, 2021
- Messages
- 3,864
- Reaction score
- 4,239
I want to harp on that last sentence as sage wisdom.i personally would not prescribe a tapering script.
Your tapering Rx can be diverted or associated with an OD.
If the latter occurs, you're gonna be in court with no leg to stand on because you prescribed to a known opiate misuser.
Don't do it.
Baclofen 10mg BID #20 with gabapentin 100mg BID #20. Don't give clonidine.
Document you managed their potential wean with the above recs.
- Joined
- Mar 4, 2007
- Messages
- 61
- Reaction score
- 12
I want to harp on that last sentence as sage wisdom.
Your tapering Rx can be diverted or associated with an OD.
If the latter occurs, you're gonna be in court with no leg to stand on because you prescribed to a known opiate misuser.
Don't do it.
Baclofen 10mg BID #20 with gabapentin 100mg BID #20. Don't give clonidine.
Document you managed their potential wean with the above recs.
Why no clonidine?
- Joined
- May 30, 2005
- Messages
- 23,349
- Reaction score
- 14,996
Z/Z 4mg tid prn #21 of each
Clonidine 0.1mg bid #14 ok
Clonidine 0.1mg bid #14 ok
- Joined
- Aug 7, 2018
- Messages
- 26
- Reaction score
- 13
Our policy is if they live in the same household, they can not be prescribed the same med for monitoring purposes. Also, if one member of the household gets discharged for violation of their opioid agreement, then anyone living in that household is also discharged.
- Joined
- Aug 28, 2019
- Messages
- 106
- Reaction score
- 190
Of course I read a thread like this and have an issue a few days later.
Inherited husband and wife couple in mid 60s. Have been seen for a decade (possibly even longer, EMR only goes so far back) in our clinic and essentially on opiates since their first visit. Wife on 10mg hydrocodone QID PRN. Doing poorly. Newish rotator cuff tear. Can't afford PT. Injection by ortho only helped for a short time. No plans for surgery apparently. Left-sided low back pain with a referral pattern down left thigh. Not conistent with radicular pain. Not big on injections since nothing has worked. Wonder what I am doing here.
Husband on oxycodone 10mg TID PRN. Pain seemingly consistent with LLE sciatica, but who knows since his last MRI was from 2013. Can't afford another MRI.
Roomed these patients separately the first time I saw them, but my schedule was overbooked so I saw them together to save time. Probably bad idea in general, but I did get to see a useful dynamic.
Interview wife as above. Like pulling teeth. Interview husband. Husband says he is doing well. Wife chimes in and says that he is too scared to ask for more or a higher dose. Give spiel that I am not increasing these doses. Red flag. Her UDS is positive for oxycodone. Still awaiting confirmation. Going to bring them in on short notice for UDS and pill count if confirmation positive. Best case scenario they both get placed on Butrans.
I could go on and on about this doctor, but neither the time nor place.
That kind of inherited couple- on the first visit- should come with templated discharge instructions, pre-approved Buprenorphine, a google review scrub, and a concealed carry permit (for you).
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
That’s a goofy policy. So someone gets oxycodone or morphine just so you can tell it’s not hydrocodone? Medication management should be a little more nuanced on when you decide what opiate is appropriate.Our policy is if they live in the same household, they can not be prescribed the same med for monitoring purposes. Also, if one member of the household gets discharged for violation of their opioid agreement, then anyone living in that household is also discharged.
- Joined
- Dec 12, 2006
- Messages
- 3,107
- Reaction score
- 3,679
I also have this policy. You'd be surprised how many couples just swap opioids like they're tylenol. When I've changed one of the two over to a different med, there is often a dirty UDS. I have also stopped meds from shared benzos. People should take their own prescribed meds, not others.That’s a goofy policy. So someone gets oxycodone or morphine just so you can tell it’s not hydrocodone? Medication management should be a little more nuanced on when you decide what opiate is appropriate.
- Joined
- Sep 14, 2009
- Messages
- 5,944
- Reaction score
- 8,267
So if someone is taking hydrocodone/APAP and they’re told they have to avoid Tylenol but they also have a morphine intolerance, and their spouse is taking oxycodone, are you going to make them switch so the first person can go on plain oxycodone?I also have this policy. You'd be surprised how many couples just swap opioids like they're tylenol. When I've changed one of the two over to a different med, there is often a dirty UDS. I have also stopped meds from shared benzos. People should take their own prescribed meds, not others.
- Joined
- May 30, 2005
- Messages
- 23,349
- Reaction score
- 14,996
always prescribe couples the same exact medication’s so they can never fail a UDS by taking each other’s drugs. You guys are so stupid.
Baclofen 10mg BID #20 with gabapentin 100mg BID #20. Don't give clonidine.
Z/Z 4mg tid prn #21 of each
Clonidine 0.1mg bid #14 ok
Can you please explain this? Didn't get a lot of opiate management training in fellowship, and have inherited too many of these patients in a short period of time. Thanks.
Shouldn’t be prescribing opioids if they’re on benzos. Contraindication.I also have this policy. You'd be surprised how many couples just swap opioids like they're tylenol. When I've changed one of the two over to a different med, there is often a dirty UDS. I have also stopped meds from shared benzos. People should take their own prescribed meds, not others.
- Joined
- Jun 16, 2021
- Messages
- 3,864
- Reaction score
- 4,239
Can you please explain this? Didn't get a lot of opiate management training in fellowship, and have inherited too many of these patients in a short period of time. Thanks.
Baclofen, gabapentin, clonidine, hydroxyzine and loperamide are commonly given for withdrawal symptoms.
I don't give clonidine bc it can drop BP, and in a pt population I already don't trust, I try to eliminate every possible thing I can that may have any possibility of side effects.
Inpatient is completely different of course. I'm speaking of outpt management.
I don't want someone popping 3, 4 or 7 clonidine and becoming hypotensive. Pts in the grip of a hard withdrawal can became erratic and impulsive. Isn't a stretch to consider they'd swallow a handful of clonidine.
That's an interesting drug BTW. It's been given for pain (epidural clonidine, and I've done stellates with local, Toradol, dex and clonidine), withdrawal, hypertension, ADHD, anxiety and even panic attacks.