Hi,
I am practicing anesthesia/pain physician in private practice.
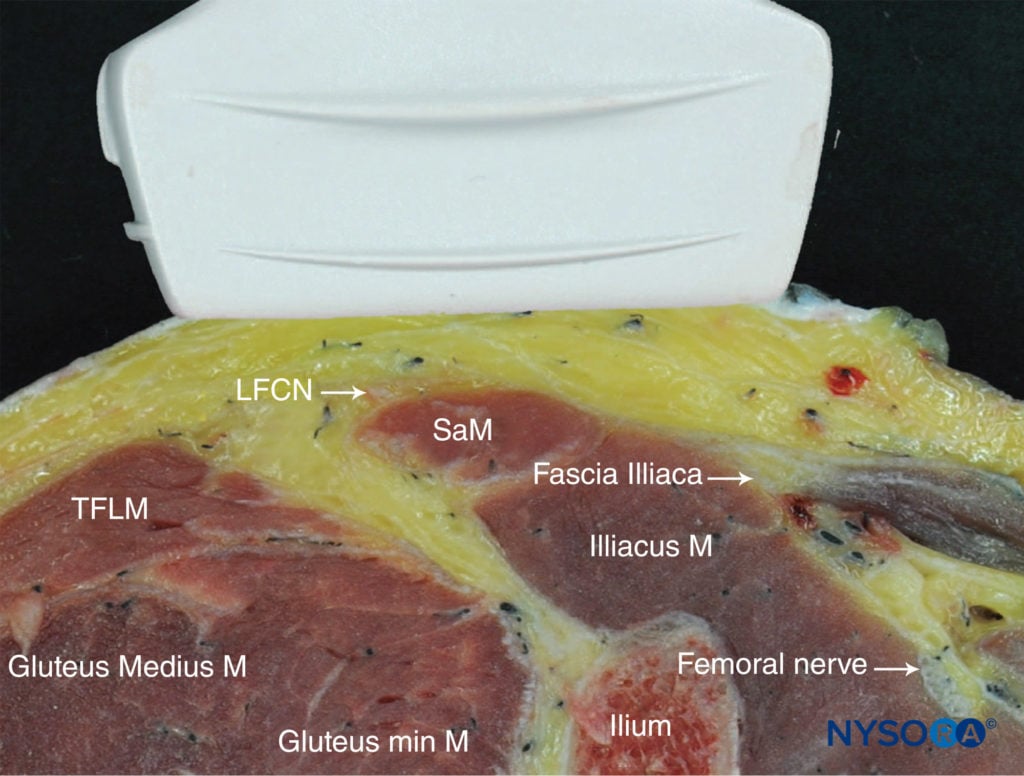
Would love to get your advice and suggestions regarding anyone experience using PHENOL for nerve ablation of lateral femoral cutaneous nerve.
If you have used what strength phenol and volume did you inject for ablation.
Thank you
Venu
I am practicing anesthesia/pain physician in private practice.
Would love to get your advice and suggestions regarding anyone experience using PHENOL for nerve ablation of lateral femoral cutaneous nerve.
If you have used what strength phenol and volume did you inject for ablation.
Thank you
Venu