I love GZ myself and this feedback makes me happy as it was one of my baby projects in the earlier part of my DE-ship. We are thinking about starting up some other types of articles that will "translate" research to practice but it needs some more time before we're ready - plus I am not EIC yet. I believe we need to provide good service to our readership which includes a lot of clinical and physics practitioners. We had to freeze GZ submissions at present because we have a backlog and I don't want them to get out of date but just to be clear, I would greatly welcome contributions of cases or responses to cases or letters to the editors about GZ cases from non-academic practitioners. In fact that's part of the overhaul which is to think of ways to enlarge the spectrum of people who participate in GZ (and the RJ in general). When we first started it (and I wrote the kickoff case), we had surgeons and medoncs participating also which I very much want to bring back as well if possible since their perspectives can be very educational. It takes a lot of coordination in its current form, so we are brainstorming ways to do this more inclusively while trying not to increase the staff burden. Thanks for the comments.@sueyom So I like RJ a lot, although I have zero publications in it myself 😆
Gray Zone is awesome. Never let that go away.
We all know it is the best dedicated radiation oncology journal.
Remember this for my next submission 😉
In all seriousness though, much respect for being the editor.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.

- Joined
- Nov 2, 2019
- Messages
- 3,601
- Reaction score
- 14,885
On that note, Sue, I do really appreciate the way you talk about Red Journal on Twitter and now on SDN. It makes it feel less like this opaque monolith of mysterious decisions.oh by the way thank you for this discussion, I am always interested in talking about RJ - any ways we can try to be better for everyone
I agree with @Ray D. Ayshun - RJ articles and features with sort of a "state-of-the-art" expert/academic approach to challenging (or even routine) cases and diseases have been great to see, and would be great to see more of.
I absolutely hate, if I'm at home or somewhere random on my phone or whatever, trying to look up a paper only to find it behind a firewall. Then I have to decide if I want to start the 6 step process of getting into my institution's VPN to see if we subscribe to that journal, only to find out we don't. At least with the ASTRO journals, I know I can log into my own account and am actually able to read the paper.
Ah, scientific publishing in 2021, ain't it grand?
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
So I like JCO a lot. I have have publications in JCO myself. It's a very appropriate venue for multidisciplinary cancer research. It's not just JCO that dominates cancer research publishing by the way, it's all the "wealthy" journals which get much more advert support from their sponsors than radonc journals get - this includes JAMA and NEJM (cardiology), Cell (biotech), etc. RJ's reach will always be restricted in a way bc it is published by small specialty society and that's reality but that doesn't mean it's a bad journal. In its present form it gives radonc a scientific and political voice - being at the top of the rankings among radiology and imaging journals is an important role for numerous complicated reasons (only a few radiology journals exceed an impact factor of 3-4). With regards to the article that was published, Dr. Brenner is an authority on radiation related risks of second malignancy and whether he is right or wrong on his numbers I think it is a good idea to start a discussion using real numbers around second malignancy risks of low dose RT to the chest (should be part of the informed consent on these COVID trials for example) and hold both sides accountable on that discussion. Just to bore you more and give a little bit more perspective, I wouldn't necessarily say that all practice changing research is off limits. I consider practice statements, contouring guidelines, discussions of fundamental radphysics/radiobio (we are a major high impact venue for this research that is very neglected by most scientific journals but is fundamental to radonc) to be practice changing in their own way - the lodestar terminology I keep in my head at all times is "practice influencing" actually. We're the only major US journal that is truly interested in FLASH or MR guided RT or RT-immunobio, or fine points of SRS/SBRT, etc. We published ASCENDE-RT and multiple secondary analyses of ASCENDE and SABR-COMET as well as the original UNC study of deintensification. I'm also okay if we're an incubator and we support the reputation and careers of people getting their concepts off the ground. So I believe there is an important place for RJ (and GJ and all our specialty society sponsored radiation oncology journals). I realize you may not like this or that article or editorial but I'd just ask that we critique the specific issue/article and not the journal itself. That is sort of harsh to all the young editors and reviewers and staff who work really hard on it every month - and I am particularly protective of our sensitive residents who are very proud to get their certificates, etc. We think a lot about everything we publish and it's never going to be perfect but again, we are trying to provide practice engaging/influencing research, support our researchers trying to advance radonc, and importantly, represent all facets of the radonc community in some of our more wide ranging discussions. Just as one last quick note, we are looking at trying to improve several sections in 2021 including Gray Zone - it does take time and resources which are in short supply.
@sueyom - thanks for discussing openly
I can tell you will be great editor in chief
The biggest issue many of us have with dr. Brennar low dose RT COVID second malignancy risk is the authorship
While he may be an expert in rad bio second malignancy modeling, we sincerely doubt that Lisa Kachnic is
it seems like ghost authorship to the vast majority of us, though I doubt there is any recall by RJ if authors attest contribution
- Joined
- Aug 20, 2014
- Messages
- 564
- Reaction score
- 959
They and most reputable journals do, but people lie on those attestations all the time. There needs to be a way to address this, but no one seems to have a good solution.@sueyom - thanks for discussing openly
I can tell you will be great editor in chief
The biggest issue many of us have with dr. Brennar low dose RT COVID second malignancy risk is the authorship
While he may be an expert in rad bio second malignancy modeling, we sincerely doubt that Lisa Kachnic is
it seems like ghost authorship to the vast majority of us, though I doubt there is any recall by RJ if authors attest contribution
- Joined
- Aug 23, 2014
- Messages
- 3,353
- Reaction score
- 6,877
If “low dose bath” is that dangerous in the chest causing all sorts of deadly secondary malignancies, most thoracic patients should be getting treated at a proton centre.
- Joined
- Oct 4, 2017
- Messages
- 5,433
- Reaction score
- 10,663
Serious question. How do we know low dose bath is bad- just by extrapolating backwards from high doses. I thought nrc recognized hormesis for low doses.If “low dose bath” is that dangerous in the chest causing all sorts of deadly secondary malignancies, most thoracic patients should be getting treated at a proton centre.
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
If “low dose bath” is that dangerous in the chest causing all sorts of deadly secondary malignancies, most thoracic patients should be getting treated at a proton centre.
agree. I don’t think low dose RT will work based on the published data now
but it’s quite clear there was a big subset of docs in radonc who didn’t believe it was worth even trying to begin with
They’ve been fearmongoring and openly trying to make our field look stupid
Ralph W, David Kirsch, Columbia clearly, etc
we all know second malignancy risk is very low after RT period but have to deal with anti RT bias from everyone else. Shame when we self flagellate ourselves openly
- Joined
- Oct 4, 2017
- Messages
- 5,433
- Reaction score
- 10,663
Would have to ignore neutron contamination with protons.If “low dose bath” is that dangerous in the chest causing all sorts of deadly secondary malignancies, most thoracic patients should be getting treated at a proton centre.
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
I know there’s a lot of Spratt haters on here but I’m a fan
at least he has cajones to stand up to the urologists when needed
at least he has cajones to stand up to the urologists when needed
- Joined
- Mar 20, 2013
- Messages
- 2,329
- Reaction score
- 4,295
I know there’s a lot of Spratt haters on here but I’m a fan
at least he has cajones to stand up to the urologists when needed
Unfortunately he deleted the thread.
Notuce that all responses against him only attacked the “tone” or appealed to the credentials of the authors.
No one questioned his actual criticism. Prostatectomy for high risk disease is more and more common....and these studies are often cited as rationale.
Dan Spratt, gym photos and all, is who this field needs. Unleash the Kraken.*
*this is hyperbole...but we need someone in rad onc brave enough to stand up and publicly call out BS studies . Twitter just as good as a letter back to the editor.
Last edited:
Thanks, that's kind to say and we will see - remains to be determined LOL.@sueyom - thanks for discussing openly
I can tell you will be great editor in chief
The biggest issue many of us have with dr. Brennar low dose RT COVID second malignancy risk is the authorship
While he may be an expert in rad bio second malignancy modeling, we sincerely doubt that Lisa Kachnic is
it seems like ghost authorship to the vast majority of us, though I doubt there is any recall by RJ if authors attest contribution
I cannot comment on LDRT secondary risks or hormesis. It is not frankly something I know enough about. I do a lot of thoracic RO myself but second malignancy is not a major consideration in a NSCLC patient. It might be a different calculus for a young coronavirus patient.
We obviously do not support gift, honorary, or guest authorships at RJ (ghost authorship is something very different). We considered instituting author declarations of contribution as many journals do, but it's unclear to us what the actual effect is and secondly our authors already complain that the submission process is too burdensome (although it is much better than most).
We take substantive complaints very seriously but a formal charge must be brought and there is a lengthy adjudication process following COPE guidelines.
- Joined
- Oct 4, 2017
- Messages
- 5,433
- Reaction score
- 10,663
I know there’s a lot of Spratt haters on here but I’m a fan
at least he has cajones to stand up to the urologists when needed
For most part, I think almost everyone here has a very favorable opinion of Dan spratt, but may not agree with him 100% of the time.
- Joined
- Nov 2, 2019
- Messages
- 3,601
- Reaction score
- 14,885
@Dan Spratt went full SDN on Twitter.Unfortunately he deleted the thread.
Notuce that all responses against him only attacked the “tone” or appealed to the credentials of the authors.
No one questioned his actual criticism.
Dan Spratt, gym photos and all, is who this field needs. Unleash the Kraken.
You never go full SDN on Twitter!
But man, if ever there was a paper to unleash on...it was that one. What garbage.
- Joined
- May 7, 2014
- Messages
- 1,779
- Reaction score
- 3,828
DId anyone preserve the original tweet?
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
Unfortunately he deleted the thread.
Notuce that all responses against him only attacked the “tone” or appealed to the credentials of the authors.
No one questioned his actual criticism. Prostatectomy for high risk disease is more and more common....and these studies are often cited as rationale.
Dan Spratt, gym photos and all, is who this field needs. Unleash the Kraken.*
*this is hyperbole...but we need someone in rad onc brave enough to stand up and publicly call out BS studies . Twitter just as good as a letter back to the editor.
DAMN! Even Spratt Censored
why I only lurk Twitter
And yes I guess that means my cajones are smaller than Spratt.
oh well
oh and also proof why SDN is needed for anonymity
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
Thanks, that's kind to say and we will see - remains to be determined LOL.
I cannot comment on LDRT secondary risks or hormesis. It is not frankly something I know enough about. I do a lot of thoracic RO myself but second malignancy is not a major consideration in a NSCLC patient. It might be a different calculus for a young coronavirus patient.
We obviously do not support gift, honorary, or guest authorships at RJ (ghost authorship is something very different). We considered instituting author declarations of contribution as many journals do, but it's unclear to us what the actual effect is and secondly our authors already complain that the submission process is too burdensome (although it is much better than most).
We take substantive complaints very seriously but a formal charge must be brought and there is a lengthy adjudication process following COPE guidelines.
thanks for response
yes I know there’s no real recall since this is just educated speculation
it’s not like any of us could prove the claims of author contributions for that specific paper but it’s about as believable as the authorship of same person on the RTOG hippocampal sparing study
don’t think enough anal cancer brain mets exist but what do I know as I’m just a humble community SDN doc
D
deleted969641
If “low dose bath” is that dangerous in the chest causing all sorts of deadly secondary malignancies, most thoracic patients should be getting treated at a proton centre.
We are worrying about secondary malignancies in COVID patients sick enough to be hospitalized to the point somebody is crazy enough to radiate their lungs and see what happens.
COVID is a disease that almost exclusively causes severe illness in the morbidly obese and elderly, many of whom have well under a 10 year life expectancy.
Secondary malignancies take about 20-30 years to manifest.
However, I am thankful for this important publication nonetheless. I am personally going back to AP-PA for my Hodgkin's patients. Wait. No. Scratch that. Just throw some more ABVD at them. We can't take chances.
- Joined
- Mar 20, 2013
- Messages
- 2,329
- Reaction score
- 4,295
DId anyone preserve the original tweet?
He just said it was a garbage study and the journal should be embarrassed about publishing it. He’s been frustrated that letters to editors complain about it but these things still get published so he was voicing his opinions on Twitter.
Though he said it better than that that was the gist of it as I remember.
He went on to cite the actual data and reasons why it was garbage but people were butt hurt over “tone” and appealed to the authority of the paper’s authors...not Spratts arguments.
...or at least that was my take.
I too am too cowardly to post on Twitter, so hats offf to to Dan and Simul et al for the BDE for rad onc . The voice of the voiceless.
- Joined
- Nov 2, 2019
- Messages
- 3,601
- Reaction score
- 14,885
He dressed it up a bit for a multi-Tweet beatdown:
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
He just said it was a garbage study and the journal should be embarrassed about publishing it. He’s been frustrated that letters to editors complain about it but these things still get published so he was voicing his opinions on Twitter.
Though he said it better than that that was the gist of it as I remember.
He went on to cite the actual data and reasons why it was garbage but people were butt hurt over “tone” and appealed to the authority of the paper’s authors...not Spratts arguments.
...or at least that was my take.
I too am too cowardly to post on Twitter, so hats offf to to Dan and Simul et al for the BDE for rad onc . The voice of the voiceless.
it was even stronger than thay
called it embarrassment to urology, prostate cancer, the authors, the journal who published it, research in general
I was in awe
- Joined
- Aug 23, 2014
- Messages
- 3,353
- Reaction score
- 6,877
Whenever i review CVs, anybody with an NCBD study as their “top” achievement, i just throw in trash!!
- Joined
- Apr 3, 2019
- Messages
- 5,005
- Reaction score
- 11,485
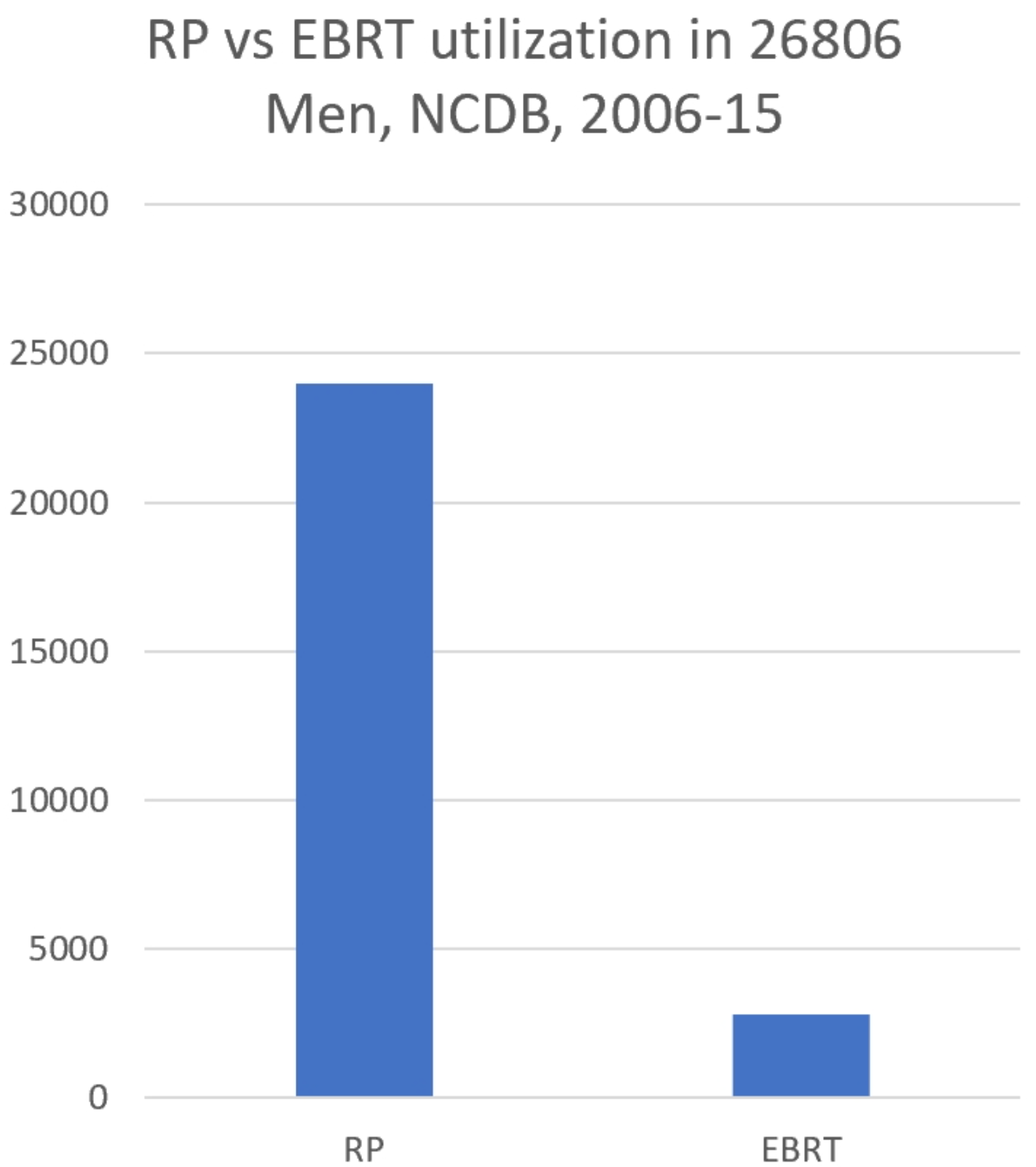
You are not kidding, this was the ratio of RP to EBRT nationally in their NCDB analysis over ~10 years. In other words they were looking at about 200 patients per year NATIONALLY getting EBRT for high risk prostate cancer. Rad onc is a good specialty as long as the urologists allow us to practice it.Prostatectomy for high risk disease is more and more common
...
On a lighter note
Last edited:
- Joined
- Apr 3, 2019
- Messages
- 5,005
- Reaction score
- 11,485
The Internet/Google is to making people into mini-private-detectives socially as NCDB analyses are to making MDs into scientists.Whenever i review CVs, anybody with an NCBD study as their “top” achievement, i just throw in trash!!
- Joined
- Nov 2, 2019
- Messages
- 3,601
- Reaction score
- 14,885
You are not kidding, this was the ratio of RP to EBRT nationally in their NCDB analysis over ~10 years. In other words they were looking at about 200 patients per year NATIONALLY getting EBRT for high risk prostate cancer. Rad onc is a good specialty as long as the urologists allow us to practice it.
...
On a lighter note
Hahaha Fuller nailed it. My obvious personal favorite:
- Joined
- Apr 28, 2005
- Messages
- 1,326
- Reaction score
- 3,776
DId anyone preserve the original tweet?
Last edited:
- Joined
- Jan 10, 2010
- Messages
- 2,753
- Reaction score
- 3,865
Resident urologist weighing in. First off, let me say I agree that another retrospective NCDB review showing improved OS with surgery over radiation is neither novel nor informative, as it does not address any of the glaring issues of selection bias from the other 5,000 NCDB reviews that have been done. It also lacks face validity (50% OS improvement makes no logical sense, or I need to start offering RP to patients as a life extending treatment for all indications).
That being said, the uproar caused in rad-onc caused by a bad article in a low rent urology journal is pretty appalling. Chairman of a program calling a paper that some resident wrote "tabloid trash" on social media is unprofessional IMO, and I usually like what Dr. Spratt writes. Even worse is the chairman below, calling for people to write letters to promotion committees to effectively end people's careers. Be better.

That being said, the uproar caused in rad-onc caused by a bad article in a low rent urology journal is pretty appalling. Chairman of a program calling a paper that some resident wrote "tabloid trash" on social media is unprofessional IMO, and I usually like what Dr. Spratt writes. Even worse is the chairman below, calling for people to write letters to promotion committees to effectively end people's careers. Be better.
- Joined
- Apr 28, 2005
- Messages
- 1,326
- Reaction score
- 3,776
You would think if you're far enough into academics and are at the point where you're reviewing or editing you just pass on something that is clearly this bad. So if you want to blame someone I would include them as well. Also, above is just Ralph being Ralph, he has somehow acquired a life long pass for saying whatever he wants on Twitter with no consequences. He's previously called out med students on Twitter for no apparent reason.
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
Resident urologist weighing in. First off, let me say I agree that another retrospective NCDB review showing improved OS with surgery over radiation is neither novel nor informative, as it does not address any of the glaring issues of selection bias from the other 5,000 NCDB reviews that have been done. It also lacks face validity (50% OS improvement makes no logical sense, or I need to start offering RP to patients as a life extending treatment for all indications).
That being said, the uproar caused in rad-onc caused by a bad article in a low rent urology journal is pretty appalling. Chairman of a program calling a paper that some resident wrote "tabloid trash" on social media is unprofessional IMO, and I usually like what Dr. Spratt writes. Even worse is the chairman below, calling for people to write letters to promotion committees to effectively end people's careers. Be better.
View attachment 336173
i understand why you feel that way @DoctwoB
The reason why this got a visceral response from Dan and others is that we already have to deal with anti-RT bias from many urologists
This study inappropriately adds ammo to the bias which is transferred to patients and forcing them to make a potentially uninformed decision over their health
being extra polite hasn’t worked for radonc thus far
I work with overall good urologists now but not everyone has that same experience, certainly not what I saw during training
Last edited:
- Joined
- Mar 30, 2009
- Messages
- 778
- Reaction score
- 1,400
We were really on the road to getting respect, no longer. Perfect story, urologist comes to a lecture where all the resident and fellows are at. He asks the med onc fellow questions and ignores all the rad onc residents (this is during the "glory days" of rad onc mind you). Now that we are returning to the dark days of rad onc, you can kiss respect good bye! Ok, maybe too much of a hyperbole, but rad onc's are always around scrapping for respect, I think we got a little, but who knows for how much longer.i understand why you feel that way @DoctwoB
The reason why this got a visceral response from Dan and others is that we already have to deal with anti-RT bias from many urologists
This just adds ammo against the bias which is transferred to patients and forcing them to make a potentially uninformed decision over their health
being extra polite hasn’t worked for radonc thus far
I work with overall good urologists now but not everyone has that same experience, certainly not what I saw during training
Here is the sad part of the story, the question the urologist asked I didn't know the answer too, but the med onc fellow did... oh what a kick in the gut LOL
For those interested
Q: What chromosome abnormality do testicular germ cell tumors show?
A: Gain of isochromosome 12p
- Joined
- Sep 20, 2004
- Messages
- 12,496
- Reaction score
- 13,040
Bingo... Even worse out in the real world with GUs trying to promote cryo and HIFU with equipoise to RTi understand why you feel that way @DoctwoB
The reason why this got a visceral response from Dan and others is that we already have to deal with anti-RT bias from many urologists
This study inappropriately adds ammo to the bias which is transferred to patients and forcing them to make a potentially uninformed decision over their health
being extra polite hasn’t worked for radonc thus far
I work with overall good urologists now but not everyone has that same experience, certainly not what I saw during training
- Joined
- Sep 20, 2004
- Messages
- 12,496
- Reaction score
- 13,040
Irony is of course i think i have seen more actual chair jobs posted this year than i have seen in a long time.... Job market is great if you're in that select applicant pool
- Joined
- Nov 2, 2019
- Messages
- 3,601
- Reaction score
- 14,885
Speaking personally, the visceral reaction this evoked in me comes from seeing the notes from my Urology colleagues at my institution and the surrounding community. Over perhaps the last 12-24 months, they have all started including a sentence (or even a blurb) in their template A&P block knocking radiation in some way (i.e. "studies have shown that EBRT, compared to RP, leads to a less durable response in prostate cancer").Resident urologist weighing in. First off, let me say I agree that another retrospective NCDB review showing improved OS with surgery over radiation is neither novel nor informative, as it does not address any of the glaring issues of selection bias from the other 5,000 NCDB reviews that have been done. It also lacks face validity (50% OS improvement makes no logical sense, or I need to start offering RP to patients as a life extending treatment for all indications).
That being said, the uproar caused in rad-onc caused by a bad article in a low rent urology journal is pretty appalling. Chairman of a program calling a paper that some resident wrote "tabloid trash" on social media is unprofessional IMO, and I usually like what Dr. Spratt writes. Even worse is the chairman below, calling for people to write letters to promotion committees to effectively end people's careers. Be better.
View attachment 336173
The "studies have shown" bit is supported in general by - you guessed it - "NCDB studies in low rent Urology journals".
High-quality studies most definitely have not shown that RP is superior to XRT in prostate cancer. However, this garbage is clearly now affecting patient care. I find that wholly unacceptable, and if it takes a Chair causing an "unprofessional" fracas on Twitter to turn the tide on this, I am 100% on board.
- Joined
- Nov 2, 2019
- Messages
- 3,601
- Reaction score
- 14,885
Perhaps one of your more senior colleagues who is involved in the ABR clinical written exams has heard this story?We were really on the road to getting respect, no longer. Perfect story, urologist comes to a lecture where all the resident and fellows are at. He asks the med onc fellow questions and ignores all the rad onc residents (this is during the "glory days" of rad onc mind you). Now that we are returning to the dark days of rad onc, you can kiss respect good bye! Ok, maybe too much of a hyperbole, but rad onc's are always around scrapping for respect, I think we got a little, but who knows for how much longer.
Here is the sad part of the story, the question the urologist asked I didn't know the answer too, but the med onc fellow did... oh what a kick in the gut LOL
For those interested
Q: What chromosome abnormality do testicular germ cell tumors show?A: Gain of isochromosome 12p
That would explain the ridiculously obscure question that was asked on boards last month about a genetic mutation in a reproductive organ tumor, which I only knew the answer to because of something I did during my PhD almost 10 years ago.
Just kidding - I know at least one of those questions shows up every year and has for the past 30 years because...why not?
- Joined
- Apr 3, 2019
- Messages
- 5,005
- Reaction score
- 11,485
It is said that there are basically only two types of horror story movie plots: one where the terror comes from the outside, and one where the terror comes from the inside. With urology not referring to rad onc and giving RT so little respect, and with our leaders gutting rad onc by continually supplying the specialty with more "fresh meat," we have one of those rare... and scary!... horror stories where both things are happening at the same time. One thing that the "tabloid trash" NCDB analysis did was show that urology does RPs vs refer for EBRT 10:1 in America (for high risk CaP no less). The study should have been a "wakeup call" to Spratt and us, but not because it was bad science; it was harsh reality.
Last edited:
- Joined
- Jan 10, 2010
- Messages
- 2,753
- Reaction score
- 3,865
Write a letter to the editor. Critique the study (but not personally attack the authors) on Twitter or in other forums. And be consistent, where were the irate diatribes on the single institution retrospective series showing EBRT plus brachy was better then xrt or RP. Personal attacks on whatever med student or resident are inappropriate and won’t bring the change you seek, nor will they affect bad actors within any field.Speaking personally, the visceral reaction this evoked in me comes from seeing the notes from my Urology colleagues at my institution and the surrounding community. Over perhaps the last 12-24 months, they have all started including a sentence (or even a blurb) in their template A&P block knocking radiation in some way (i.e. "studies have shown that EBRT, compared to RP, leads to a less durable response in prostate cancer").
The "studies have shown" bit is supported in general by - you guessed it - "NCDB studies in low rent Urology journals".
High-quality studies most definitely have not shown that RP is superior to XRT in prostate cancer. However, this garbage is clearly now affecting patient care. I find that wholly unacceptable, and if it takes a Chair causing an "unprofessional" fracas on Twitter to turn the tide on this, I am 100% on board.
- Joined
- Apr 3, 2019
- Messages
- 5,005
- Reaction score
- 11,485
As prostate cancer incidence has significantly fallen over last decade, I have seen the urologists' desire to do RP increase. Kindness or abrasiveness on Twitter won't affect human behavior all that much. Human behavior is best studied, and affected, via a scientific field called economics.Write a letter to the editor. Critique the study (but not personally attack the authors) on Twitter or in other forums. And be consistent, where were the irate diatribes on the single institution retrospective series showing EBRT plus brachy was better then xrt or RP. Personal attacks on whatever med student or resident are inappropriate and won’t bring the change you seek, nor will they affect bad actors within any field.
D
deleted969641
I'm not sure you know what a "personal attack" is. Am I personally attacking you right now? Maybe. Maybe I don't know what a personal attack is either. I would think it would require me personally knowing something about you. But Dan Spratt's response in calling out that pile of detritus was correct and appropriate and he shouldn't have deleted it. The trick of calling something that threatens you "unprofessional" in order to shut down debate is s.o.p. in academics. No, it's not unprofessional to call out academic dishonesty, which is what that article is. It's about as close to outright falsifying data as you can get.Write a letter to the editor. Critique the study (but not personally attack the authors) on Twitter or in other forums. And be consistent, where were the irate diatribes on the single institution retrospective series showing EBRT plus brachy was better then xrt or RP. Personal attacks on whatever med student or resident are inappropriate and won’t bring the change you seek, nor will they affect bad actors within any field.
- Joined
- Jan 10, 2010
- Messages
- 2,753
- Reaction score
- 3,865
Please, don’t insult me. Disagreement is not attack. Calling someone’s work a pile of trash isn’t great, even if you don’t use their name so we could quibble on the semantics there. Not is it necessary, as one can critique using language compatible with professional discourse. To that end, see Dr. Spratts updated critique (the previous is deleted) which I have no problems with and raises valid points.I'm not sure you know what a "personal attack" is. Am I personally attacking you right now? Maybe. Maybe I don't know what a personal attack is either. I would think it would require me personally knowing something about you. But Dan Spratt's response in calling out that pile of detritus was correct and appropriate and he shouldn't have deleted it. The trick of calling something that threatens you "unprofessional" in order to shut down debate is s.o.p. in academics. No, it's not unprofessional to call out academic dishonesty, which is what that article is. It's about as close to outright falsifying data as you can get.
Calling for people to write their promotion committee to deny promotion or lose his job is undoubtedly a personal attack and inappropriate.FWIW I agree the term professionalism is sometimes inappropriately used to silence discourse we don’t agree with. This is not one of those times. We should have SOME standards for how we conduct ourselves as physicians.
- Joined
- Oct 10, 2011
- Messages
- 8,963
- Reaction score
- 11,453
For all the RJ bashing, give credit to @sueyom that something in-line with the that garbage study published in urologic oncology will not cross RJ's shores in 2021 and onwards.
I agree with you on critiquing the paper and not personally attacking the first author, who is probably a medical student and likely does not know any better.
However, I do think that calling out the senior author for publishing trash research which has the ability to harm patients (per people 'citing' it in consult notes as per above) is a reasonable thing a chairman can do. Yes, it's aggressive and not 'nice' but I am personally OK with Rad Oncs in position of power to be able to do it. One can whine about being unprofessional, but IMO it's an existential threat to Rad Onc about the increase in rate of RP use in high-risk PCa now compared to 10 or 15 years ago. Doubly so for Dan Spratt who is GU only (maybe even prostate only) when it comes to Rad onc.
The single institution series showing EBRT + brachy better than XRT or RP is actually a multi-institutional retrospective review from 12 institutions. Here is the link Disease Progression and Mortality in Gleason 9-10 Prostate Cancer After Definitive Treatment
It does not replace clinical trial and I hope that a rad onc would not use that as 'justification' to recommend EBRT + brachy compared to XRT or RP for a survival benefit in a consultation note.
First off, ASCENDE-RT suggests that there is some benefit of adding brachy to XRT in a randomized trial. We can discuss whether bPFS is sufficient or whether DMFS is necessary. Kishan et al is suggesting that a higher subset of patients than those who were enrolled in ASCENDE-RT may show a survival benefit. We know from Miccio et al (Quantifying treatment selection bias effect on survival in comparative effectiveness research: findings from low-risk prostate cancer patients) that treatment selection bias is a huge issue that can frequently drive OS. But it is in favor of RP > EBRT + BT > EBRT. So the fact that EBRT + BT is better than EBRT may just be treatment selection bias (or at least in part). But for EBRT + BT to be better than RP is unlikely to be treatment selection bias. It might just be the ADT that helps reduce distant metastasis free survival. But maybe it is the radiation.
Write a letter to the editor. Critique the study (but not personally attack the authors) on Twitter or in other forums. And be consistent, where were the irate diatribes on the single institution retrospective series showing EBRT plus brachy was better then xrt or RP. Personal attacks on whatever med student or resident are inappropriate and won’t bring the change you seek, nor will they affect bad actors within any field.
I agree with you on critiquing the paper and not personally attacking the first author, who is probably a medical student and likely does not know any better.
However, I do think that calling out the senior author for publishing trash research which has the ability to harm patients (per people 'citing' it in consult notes as per above) is a reasonable thing a chairman can do. Yes, it's aggressive and not 'nice' but I am personally OK with Rad Oncs in position of power to be able to do it. One can whine about being unprofessional, but IMO it's an existential threat to Rad Onc about the increase in rate of RP use in high-risk PCa now compared to 10 or 15 years ago. Doubly so for Dan Spratt who is GU only (maybe even prostate only) when it comes to Rad onc.
The single institution series showing EBRT + brachy better than XRT or RP is actually a multi-institutional retrospective review from 12 institutions. Here is the link Disease Progression and Mortality in Gleason 9-10 Prostate Cancer After Definitive Treatment
It does not replace clinical trial and I hope that a rad onc would not use that as 'justification' to recommend EBRT + brachy compared to XRT or RP for a survival benefit in a consultation note.
First off, ASCENDE-RT suggests that there is some benefit of adding brachy to XRT in a randomized trial. We can discuss whether bPFS is sufficient or whether DMFS is necessary. Kishan et al is suggesting that a higher subset of patients than those who were enrolled in ASCENDE-RT may show a survival benefit. We know from Miccio et al (Quantifying treatment selection bias effect on survival in comparative effectiveness research: findings from low-risk prostate cancer patients) that treatment selection bias is a huge issue that can frequently drive OS. But it is in favor of RP > EBRT + BT > EBRT. So the fact that EBRT + BT is better than EBRT may just be treatment selection bias (or at least in part). But for EBRT + BT to be better than RP is unlikely to be treatment selection bias. It might just be the ADT that helps reduce distant metastasis free survival. But maybe it is the radiation.
D
deleted969641
If you believe that the article represents academic dishonestly, which I feel that it clearly does (as it suggests a conclusion not supported by reality which could lead to patient harm), then that is the appropriate action. Reprimands are appropriate in cases of academic dishonestly. This is so blatant that a outright retraction is warranted along with an apology from the authors.Calling for people to write their promotion committee to deny promotion or lose his job is undoubtedly a personal attack and inappropriate.
Can you imagine the fallout if a rad onc did the exact same thing with SBRT vs lobectomy or god forbid, upfront SRS vs. crainotomy and GTR? I promise you the neurosurgeons wouldn't be deleting tweets and rephrasing them more nicely with emojis and winky faces.
Edit: Just for reference, I always discuss surgery with my prostate patients and even will encourage some younger men with high risk cancer to consider it as long as they are aware of their outcome nomogram-based odds. I understand wanting to avoid ADT. I've been mostly lucky in working with urologists who feel the same way and always discuss radiation with low and intermediate risk patients as well.
- Joined
- Apr 3, 2019
- Messages
- 5,005
- Reaction score
- 11,485
How many randomized trials are there looking at surgery/RT combos in breast cancer? Fifty?
And how many in prostate? Essentially zero?
Oncology is sexist.
And how many in prostate? Essentially zero?
Oncology is sexist.
- Joined
- Oct 10, 2011
- Messages
- 8,963
- Reaction score
- 11,453
Please, don’t insult me. Disagreement is not attack. Calling someone’s work a pile of trash isn’t great, even if you don’t use their name so we could quibble on the semantics there. Not is it necessary, as one can critique using language compatible with professional discourse. To that end, see Dr. Spratts updated critique (the previous is deleted) which I have no problems with and raises valid points.
Calling for people to write their promotion committee to deny promotion or lose his job is undoubtedly a personal attack and inappropriate.FWIW I agree the term professionalism is sometimes inappropriately used to silence discourse we don’t agree with. This is not one of those times. We should have SOME standards for how we conduct ourselves as physicians.
The issue with Ralph Weischelbaum is one that is well known in Rad Onc circles as well. RW is an asshat that most on this forum have an issue with not unfrequently whenever he does tweet. I think an attending losing their job or not getting promoted because of an article like this is an over-the-top response. I don't have a strong of an opinion as Turaco does above that this is 'academic dishonesty' in the same line as cheating or something.
D
deleted969641
I don't have an issue with letting this go if the authors retract it and write an explanation with an apology and extend an olive branch. Careers don't need to be impacted over that. Forgive and forget. However, if they want to double down and stick to their guns that this is 100% legit, then the gloves should come off and they should be willing to accept any criticism and debate it off rather than going to whine to their chair and get critical tweets taken down for being "unprofessional." That's antithetical to the spirit of academics (although like Ralph says not surprising). Never thought I'd be agreeing with RW...The issue with Ralph Weischelbaum is one that is well known in Rad Onc circles as well. RW is an asshat that most on this forum have an issue with not unfrequently whenever he does tweet. I think an attending losing their job or not getting promoted because of an article like this is an over-the-top response. I don't have a strong of an opinion as Turaco does above that this is 'academic dishonesty' in the same line as cheating or something.
- Joined
- Jan 10, 2010
- Messages
- 2,753
- Reaction score
- 3,865
Academic dishonesty seems strong. A med student analyzed a database and it gave a result you don’t like and they published it while noting caveats in their paper. Unless there is falsification it is not dishonest. There are many reasons to be critical of it and the entire system we live in which rewards publication quantity and not quality. But you’re hatin on a player when you should be hatin the game.
- Joined
- Nov 20, 2008
- Messages
- 165
- Reaction score
- 237
Academic dishonesty seems strong. A med student analyzed a database and it gave a result you don’t like and they published it while noting caveats in their paper. Unless there is falsification it is not dishonest. There are many reasons to be critical of it and the entire system we live in which rewards publication quantity and not quality. But you’re hatin on a player when you should be hatin the game.
Database studies are notorious for statistical issues. I have seen many errors with NCDB database studies with patient selection and not excluding outliers. What is more shocking is that you can find similar NCDB analyses with different conclusions based on the authors speciality.
I am unsure if this specific journal has an outside stats review of the results, but this should be standardized for all database studies. Furthermore, database studies should be hypothesis generating and not change the standard of care. We should use database studies to help support phase 3 trial design.
I personally like to avoid speaking ill of people when it is easy enough to trash their poor experimental design in an editorial (as you mentioned)... but I gotta say, for Harvard faculty to use a term "emulated clinical trial" in the title, he's asking for it.Academic dishonesty seems strong. A med student analyzed a database and it gave a result you don’t like and they published it while noting caveats in their paper. Unless there is falsification it is not dishonest. There are many reasons to be critical of it and the entire system we live in which rewards publication quantity and not quality. But you’re hatin on a player when you should be hatin the game.
- Joined
- Feb 11, 2005
- Messages
- 601
- Reaction score
- 483
Is it academic dishonesty or ignorance ? I would assume the latter. A letter to the editors is the polite, and academically appropriate approach. The reality is that people (urologists) will cite the study and be unaware of the letter (or simply not care about it). Dan Spratt's 1st tweet hit the nail on the head, but the revised one is more appropriate for someone in a leadership position. Lemmiwenks or MROGA are perhaps better options to call out a study as trash.
- Joined
- Apr 8, 2021
- Messages
- 201
- Reaction score
- 607
Write a letter to the editor. Critique the study (but not personally attack the authors) on Twitter or in other forums. And be consistent, where were the irate diatribes on the single institution retrospective series showing EBRT plus brachy was better then xrt or RP. Personal attacks on whatever med student or resident are inappropriate and won’t bring the change you seek, nor will they affect bad actors within any field.
calm down buddy. Nobody directly attacked the student or attending
Ralph W made an asinine comment which was unfortunate and it was 1 person
Inappropriate to label 99% of the valid criticism as nonsense bc of 1 bad actor
similarly I wouldn’t say all urologists are bad
The difference beteeen the EBRT + brachy paper is
1) patient has already chosen RT if they ever reach this point so it doesn’t affect surgical volume
2) more than half of us don’t even do brachy boost so this doesn’t change any patterns of care
3) based on the offending study being discussed, the amount of RP is so much higher than RT that clearly that other paper didn’t do any damage
Last edited:
- Joined
- Jan 10, 2010
- Messages
- 2,753
- Reaction score
- 3,865
No arguments here. “emulated clinical trial” is a bit much.
Maybe I’m just a skeptic but I think 90%+ of published research is BS. And this BS follows trends. Some of the current tends are HSR disparities (X race/gender has a different outcome then Y in database C despite controlling for two other variables) and HSR outcomes studies like the current one. Both of these show correlation despite trying to hint at causation and are hypothesis generating at best. So my response to an article like this is a collective shrug. You’ll see the same in every low end journal every month.
Maybe I’m just a skeptic but I think 90%+ of published research is BS. And this BS follows trends. Some of the current tends are HSR disparities (X race/gender has a different outcome then Y in database C despite controlling for two other variables) and HSR outcomes studies like the current one. Both of these show correlation despite trying to hint at causation and are hypothesis generating at best. So my response to an article like this is a collective shrug. You’ll see the same in every low end journal every month.