- Joined
- Oct 10, 2011
- Messages
- 9,017
- Reaction score
- 11,524
- Points
- 8,831
- Attending Physician
Advertisement - Members don't see this ad
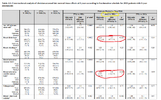
Why would anal cancer cells a/b be lower than 10? Squamous cell, concern for fast repopulation, etc. etc. A/b 10 seems appropriate.5 x 6 Gy gives a BED of 48 Gy (a/b=10 Gy)
28 x 1.8 Gy gives a BED of 59.5 Gy (a/b=10 Gy)
a/b for anal cancer cells is however perhaps lower than 10 Gy?
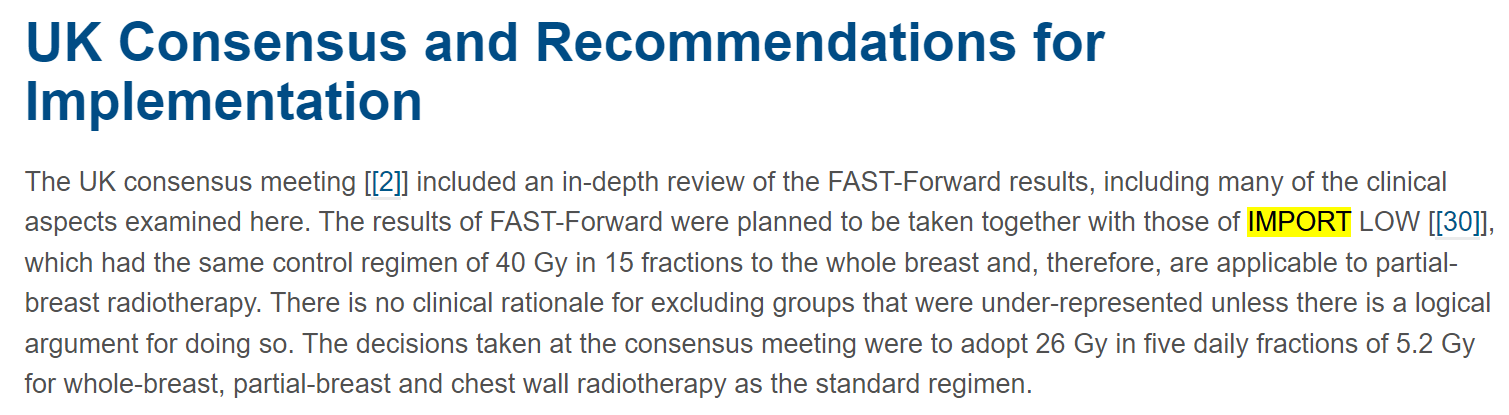
IMPORT-LOW…
So hot in quality and evidence
So cold in the heart and mind of the American MD
Nothing wrong with IMPORT-LOW, but nothing wrong with Livi et al. Different strokes for different folks.