- Joined
- Jul 6, 2004
- Messages
- 1,977
- Reaction score
- 563
Had a young patient (56 yo) who had prostatectomy last year for Gleason 3+4 with low PSA in early ‘21. He had positive margin at the right base on path and had SVI bilaterally. PSA was negative after surgery for 5 measurements then rose to detectable but still low at .05 then .06 a couple months later. He had a PSMA which was negative and was referred to talk about early salvage. Fairly anxious patient who very much wanted RT. Urology sent him to a med onc too, bc of such low PSA they opted against ADT.
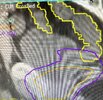
I sim’d him and of course he has a loop of small bowel hanging very low (lot of bowel in general low), I did 4500 and conedown to 7020 as superior as I could while staying within tolerance. I fused the pre surgical MRI and where the base (and majority of SV) were aren’t covered in the 7020, more like 5500 at the low base and 4500 at the high base (median lobe that pushed into the bladder)
Appreciate thoughts on management, would you just proceed as is and maybe ask med onc to reconsider ADT. I don’t think prone is going to get that bowel out of there it is pretty down behind the bladder.
I sim’d him and of course he has a loop of small bowel hanging very low (lot of bowel in general low), I did 4500 and conedown to 7020 as superior as I could while staying within tolerance. I fused the pre surgical MRI and where the base (and majority of SV) were aren’t covered in the 7020, more like 5500 at the low base and 4500 at the high base (median lobe that pushed into the bladder)
Appreciate thoughts on management, would you just proceed as is and maybe ask med onc to reconsider ADT. I don’t think prone is going to get that bowel out of there it is pretty down behind the bladder.
Last edited: