- Joined
- Jul 6, 2005
- Messages
- 283
- Reaction score
- 64
Would anyone inject? Patient with bilateral leg weakness.

Some more info....patient on prasurgel and 2 MIs two months ago with stent placement....
IMO - Caudal only if a pt is fused to the sacrum.
Otherwise bilateral S1 TFESI for lower lumbar severe stenosis, or if higher level (I usually see this between L2-3 to L4-5) I do one level below.
I think a caudal is a POS injxn. I do them, but incredibly hit or miss for me.
Bilateral S1 is far superior than a caudal in my experience.
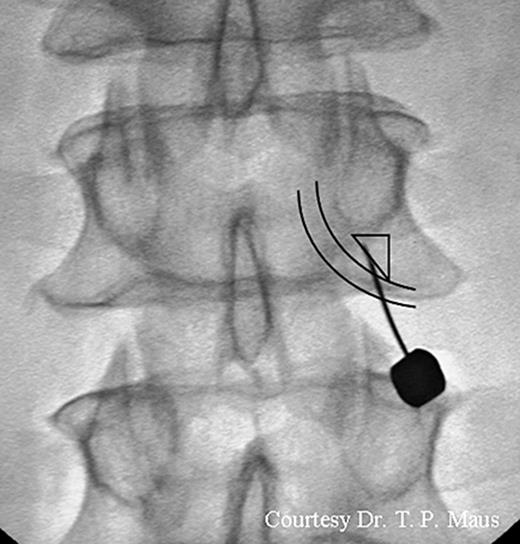
A few older pics. I'm using more ipsilateral obliquity and that's getting me a more medially oriented needle and maybe better pics but results are good enough when I was doing straight AP. I strongly recommend S1 over caudal unless the pt is fused to sacrum and you can't see the S1 foramen (you can still walk it in without seeing it though).
No lateral means you were never there.
Did the sis guidelines change to now recommend depo for lumbar TFESI?I see this everyday or at least weekly. I always do IL a level below typically. Urgent surgery referral is only if bowel/bladder dysfunction, severe sudden weakness (ie footdrop or flaccid paralysis), sudden ED in relation to this pain, etc.
But typically, I see a lot of old patients, and they all have weakness/stiffness and severe stenosis. I doubt 80 year old wants surgery. I explain risk, alternative, and benefit everyday with everyone. Alternatives include 1) Doing nothing and living with it, 2) PT and Oral Meds, 3) Epidural from me, and 4) Surgery.
I never do TFESI with these stenotic patients - I don't feel like it works because IMO Dex doesn't do anything for them, I never get good results with it. I feel like they do better with Depo. Not ballsy enough to do TFESI with Depo as per SIS Guidelines. I've always thought about doing a large study with this. My theory that I postulate is that TFESI with Dex works for more younger people, disc herniation, etc. When its elderly with stenosis, doesn't do poo diddly squat. Washes right in and out. But perhaps I am wrong, who knows, I am always open to new ideas and being wrong.
Did the sis guidelines change to now recommend depo for lumbar TFESI?
Agree that while del may work for radiculopathy, it rarely provides sustained relief in stenosis. Two different processes.
To my knowledge, nope. I don't think that'll ever change either. Just Dex for TFESI. I can never risk it. One time, while doing a TFESI, I used Kambin's approach for the infra-neural approach that is safer. I was in a vessel. Yes. A vessel, the very thing this method is supposed to avoid. Everyone's anatomy is different I've realized after that.
To my knowledge, nope. I don't think that'll ever change either. Just Dex for TFESI. I can never risk it. One time, while doing a TFESI, I used Kambin's approach for the infra-neural approach that is safer. I was in a vessel. Yes. A vessel, the very thing this method is supposed to avoid. Everyone's anatomy is different I've realized after that.
To my knowledge, nope. I don't think that'll ever change either. Just Dex for TFESI. I can never risk it. One time, while doing a TFESI, I used Kambin's approach for the infra-neural approach that is safer. I was in a vessel. Yes. A vessel, the very thing this method is supposed to avoid. Everyone's anatomy is different I've realized after that.
 academic.oup.com
academic.oup.com


