Suboxone treatment agreements should require the cessation and tapering off all addictive substances. Opioid dependence untreated carries risk of an overdose death. I believe sound practice is stopping addictive substances in patients with addictive disorders - this means stimulants, benzos, and GABA sleep agents (ambien/lunesta/sonata).
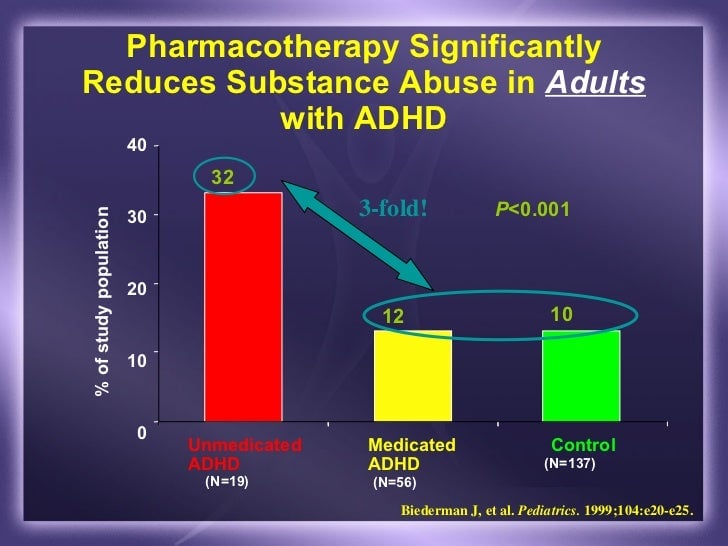
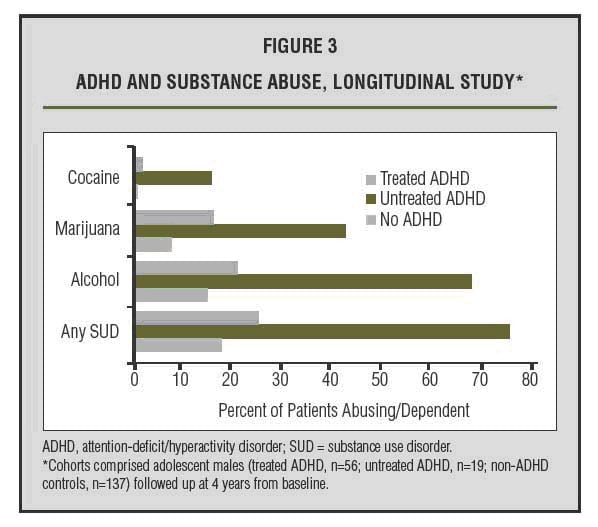
As was mentioned, there is real and hard data showing some medications can help patients get off of illicit substances that are potential substances of abuse. ADHD left untreated could make problems worse.
Heck, Suboxone is an opioid. You want them off of all addictive substances, if your comments are taken literally, take them off the Suboxone.
That said, where is the exact hard-line differs among clinicians, and I'll completely admit has changed compared to the first year I was prescribing this medication. The evidenced-based medicine only teaches us so much. We're going to get cases that don't cleanly fit in the studies. My own opinions on how to administer treatment have changed over the years I've prescribed this medication.
If a clinican had a completely hardline with no other substances no matter what, I wouldn't think they were doing bad practice. I'd disagree, but it'd be a respectful disagreement. Some patient IMHO respond better to doctors putting the rules out in such a manner.
Personally, I allow for stimulants if taken legally, with psychological testing backing they have ADHD with a trial of a nonstimulant first.
As for the Suboxone-only treatment, refer out for everything else, this is something that has never been legally challenged, but it defeats the purpose of being a physician. If you believe treatment should only be one-disorder specific (edit: with only one specific medication given, nothing else), you could have technicians with a few weeks of training give out Suboxone. Methadone clinics IMHO are an exception because they are designed to not have doctors see the patients daily, and yes, they have techs or nurses dispense the medication.
The argument of "we warned you ahead of time that I'm not really treating you as a patient, I'm treating the disorder, so it's alright." Again, never been challenged formally specifically with Suboxone, but I don't agree with that, and I can tell you this. Legally, if you have a doctor patient relationship, well guess what?
You got a doctor patient relationship. You have a fiduciary responsiblity to the patient.
Similar issues have been debated within the APA and AAPL in regards to what constitutes a doctor patient relationship (cause forensic psychiatrists, doing an evaluation for the court is not considered creating a doctor/patient relationship). I'd bet 100% of any doctors on an ethics panel would consider Suboxone treatment as creating a D-P relationship. Cutting yourself off doing what a doctor is supposed to do for a patient, if you specialize in the area where they need help, sounds unethical to me, and is not compatible with a D-P relationship.
Suboxone patients I've had with non-opioid psychiatric problems, I have treated, and offered they go to another doctor only if they needed to be seen more than monthly and we didn't accept their insurance because I wanted them to save money. If they wanted me to treat it all by myself, I would have.