
- Joined
- Dec 17, 2007
- Messages
- 3,391
- Reaction score
- 4,410
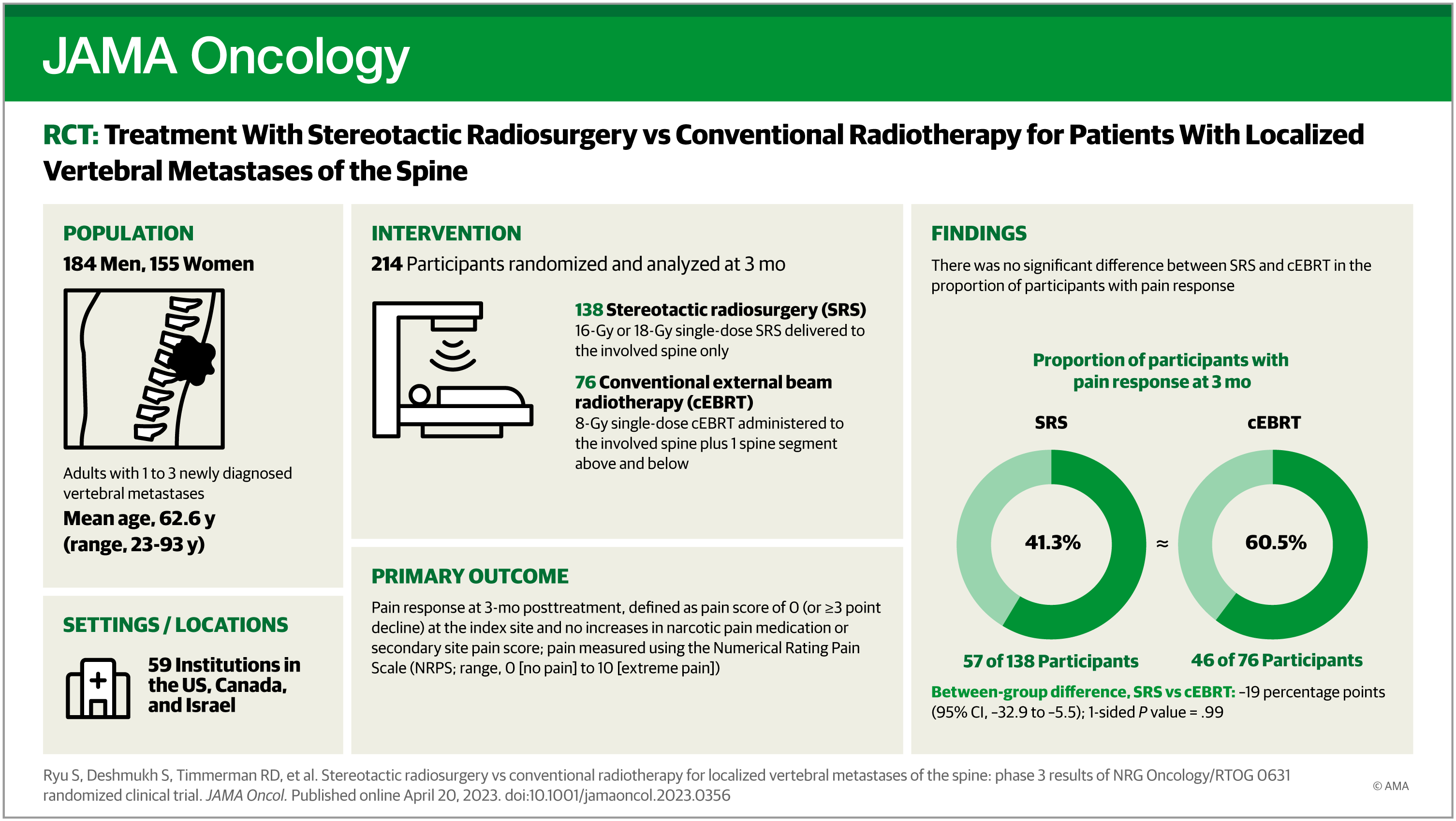
Radiosurgery of Spine Metastasis—NRG/RTOG 0631 RCT Final Results
This randomized clinical trial assesses whether patient-reported pain relief was improved with stereotactic radiosurgery compared with conventional external beam radiotherapy for patients with 1 to 3 sites of vertebral metastases.
 jamanetwork.com
jamanetwork.com
DISCUSS!

