This is a new SDN account because my original one from when SDN started was archived - I haven't been on here in some time. Full transparency - I’m a doc and high level leader with USACS and have been with the group through my legacy company since 2010. I have worked in multiple states and with multiple divisions within USACS - I’ve served at all levels of our group and I believe in our perpetual physician owned model and our ability to create programs that support our people. I also started my career as an Asst. Prof in a very well-regarded EM program in Philly, so USACS is not all that I have known.
While I’m not here to get in the mud, I do want to correct some facts about our programs and the math about an RVU model. I do not know which site the OP is looking at, but am happy to connect with anyone about our company here or privately.
This fall we launched a Physician Loan Payback (PLP) program at over 80 sites. As a physician owned company, we recognized that our current owners and newest partners were coming out of residency with tremendous debt coupled with an exceptionally unfavorable refinance environment - which we all know has gotten worse in the past few months. We are not PSLF eligible, so we chose to invest in our people. The PLP is open to our current team members at these sites as well as our new hires.
The PLP program has you refi/consolidate to a 15 year loan or you can bring a current loan with you. We have a rate reduction with Laurel Road, but the doc is free to use any bank. The doc pays for 7 years and we then pay them the balance PLUS gross-up the estimated tax burden for that payment. No cap to the amount of student loan debt that can be brought into the program. The commitment is 4 years at the initial site (or transfer to another included site during that time), then if life changes, they can transfer to any one of our 500+ sites nationwide for the final 3 years of the commitment. Leave before 7 years? No handcuffs - we wish you well.
If the PLP program doesn’t fit your needs, we are offering $150K sign-on bonus for the same sites with a 3 year commitment.
As for comp rates - our busy sites on a hybrid hourly/RVU model typically make at least twice the hourly as an average. I don’t know the site the OP has interviewed at, so cannot really comment if the rate of $170/hr is accurate, but that sounds low to me with that acuity level. I wonder if that is the lowest person at the site or a part-time doc?? Would always recommend asking what the range is at the site between high and low performers.
The comp change the OP described absolutely is a RAISE - they are decreasing hourly by $4/hr and increasing RVUs by $3/RVU. OP stated that there is a 40% admit rate at this site - so we can assume a high acuity - lets assume 4.5 RVU/pt - could even be higher with that acuity level.
At 1 pt/hr that is a $9.50/hr raise - 4.5 RVU/hr * $3/RVU = $13.50/hr - $4/hr = $9.50/hr
At 2 pt/hr that is a $23/raise - 9 RVU/hr * $3/RVU = $27/hr - $4/hr = $23/hr
They likely see 1.8-2.1 pt/hr. So unless I am missing something - this site is getting a pretty significant raise of > $20/hr.
OP - you should ask what the RVU/pt and RVU/hr at the site is to help you determine comp - as well as asking for the range of team members. The director should easily be able to show you each doc's monthly productivity as we openly share this online. Each member of a team can see their own patients/coding as well as the entire groups productivity each month.
Additionally, our compensation includes $45-50K/year in pre-tax benefits - we like our pre-tax dollars:
* 10% company contribution to 401K (not a match) up to $33K/yr in 2023 - increases each year with the increase in IRS limits
* Low cost health/dental/vision with good coverage
* STD/LTD own occupation paid for by the group
* Business expense account $4K/yr with additional $4K in the first year out of residency
* Fully paid military leave
*.Fully paid parental leave open to all new parents including adoptive (up to 12 weeks for birth moms)
* $75K equity grant at 2 year anniversary with no buy-in (yes - the IRS has you pay the taxes on this)
* Stock price has more than doubled in the past 7 years and we have at least annual opportunities to buy/sell
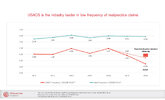
And our docs are SUED LESS THAN HALF the national average for EM because we focus on hiring high quality BCEM and actively manage our own risk.
I wish the OP the best of luck with their decision and am happy to connect if I can be of help.