
- Joined
- Nov 21, 1998
- Messages
- 12,579
- Reaction score
- 6,991
Long-term Risk of Overdose or Mental Health Crisis After Opioid Dose Tapering
This cohort study assesses the longer-term risks of overdose or mental health crisis associated with opioid dose tapering.
 jamanetwork.com
jamanetwork.com
Original Investigation Pharmacy and Clinical Pharmacology
June 13, 2022
Long-term Risk of Overdose or Mental Health Crisis After Opioid Dose Tapering
Joshua J. Fenton, MD, MPH1,2; Elizabeth Magnan, MD, PhD1,2; Irakis Erik Tseregounis, PhD3; et alGuibo Xing, PhD2; Alicia L. Agnoli, MD, MPH, MHS1,2; Daniel J. Tancredi, PhD2,4
Author Affiliations Article Information
JAMA Netw Open. 2022;5(6):e2216726. doi:10.1001/jamanetworkopen.2022.16726
editorial comment icon Editorial
Comment
Key Points
Question Is opioid dose tapering associated with reduced longer-term risks of overdose, withdrawal, or mental health crisis in patients prescribed long-term opioids?
Findings In this cohort study of 19 377 patients, in a posttaper period (beginning at least 12 months and extending up to 24 months after taper initiation) vs the pretaper period, the adjusted incidence rate ratios were 1.57 for overdose-withdrawal and 1.52 for a mental health crisis. Both were significant.
Meaning These findings suggest that opioid dose tapering was associated increased risks of overdose-withdrawal and mental health crisis that persisted up to 2 years after taper initiation.
Abstract
Importance Patients prescribed long-term opioid therapy are increasingly undergoing dose tapering. Recent studies suggest that tapering is associated with short-term risks of substance misuse, overdose, and mental health crisis, although lower opioid dose could reduce risks of adverse events over the longer term.
Objective To assess the longer-term risks of overdose or mental health crisis associated with opioid dose tapering.
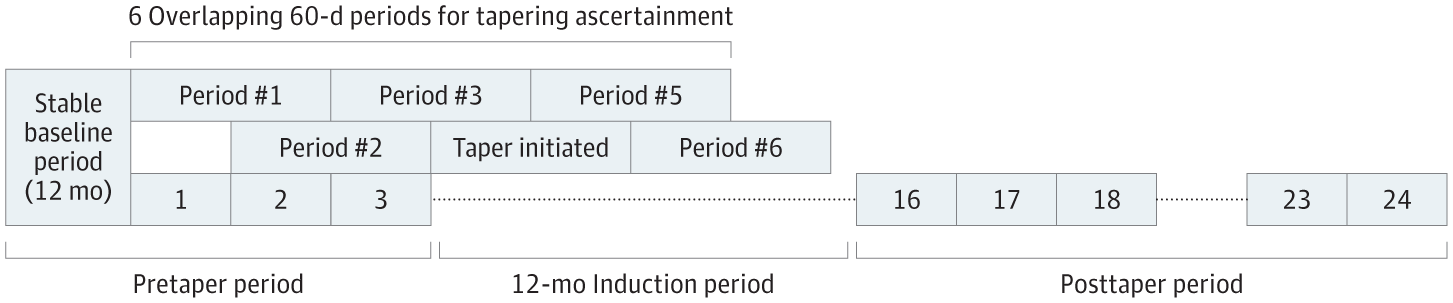
Design, Setting, and Participants This is a cohort study using an exposure-crossover analysis. Data were obtained from the OptumLabs Data Warehouse, which includes deidentified medical and pharmacy claims and enrollment records for commercial insurance and Medicare Advantage enrollees, representing a diverse mixture of ages, races, ethnicities, and geographical regions across the US. Participants were US adults who underwent opioid dose tapering from 2008 to 2017 after a 12-month baseline period of stable daily dosing of 50 morphine milligram equivalents or higher and who had at least 1 month of long-term follow-up during a postinduction period beginning 12 months after taper initiation. Data analysis was performed from October 2021 to April 2022.
Exposures Opioid tapering, defined as 15% or more relative reduction in mean daily dose during any of 6 overlapping 60-day windows within a 7-month follow-up period after the stable baseline period.
Main Outcomes and Measures Emergency or hospital encounters for drug overdose or withdrawal and mental health crisis (depression, anxiety, or suicide attempt). Outcome counts were assessed in pretaper and postinduction periods (from 12 to 24 months after taper initiation).
Results The study included 21 515 tapering events among 19 377 patients with a mean (SD) of 9.1 (2.7) months of postinduction follow-up per event (median [IQR], 10 [8-11] months). Patients had a mean (SD) age of 56.9 (11.2) years, 11 581 (53.8%) were female, and 8217 (38.2%) had commercial insurance (vs Medicare Advantage). In conditional negative binomial regression analyses, adjusted incidence rate ratios for the postinduction period compared with the pretaper period were 1.57 (95% CI, 1.42-1.74) for overdose or withdrawal and 1.52 (95% CI, 1.35-1.71) for mental health crisis.
Conclusions and Relevance These findings suggest that opioid tapering was associated with increased rates of overdose, withdrawal, and mental health crisis extending up to 2 years after taper initiation.
