- Joined
- Apr 30, 2021
- Messages
- 619
- Reaction score
- 193
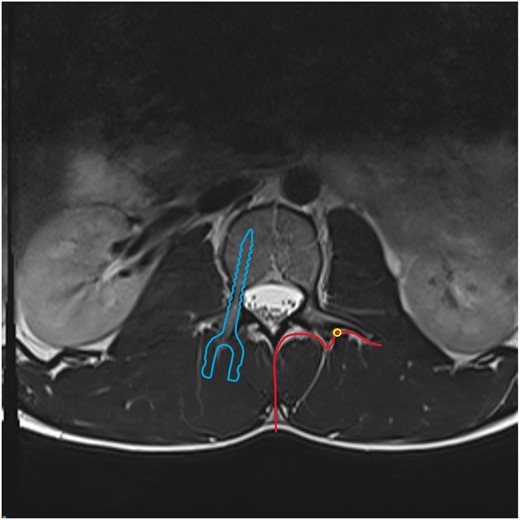
May be basic question but let’s say you were going to do treat adjacent level facets and you saw this fusion.
Where would you place your needle for diagnostic medial branch nerve block (please clarify if you’re referring to the nerve or the vertebral body on which medial branch courses)

Where would you place your needle for diagnostic medial branch nerve block (please clarify if you’re referring to the nerve or the vertebral body on which medial branch courses)