Theoretically speaking, high FiO2 (>70%) leads to more oxidative stress (reactive oxygen species generation) on the body and can contribute to atelectasis via nitrogen washout.
Since we specifically mentioned healthy adults (there is evidence that hyperoxygenation in strokes and MIs leads to worse outcomes, so literature wise, placing every chest pain patient on supplemental O2, regardless of SpO2 is out of favor, but it's just hard to kill MONA), there is evidence that it doesn't really matter as much in the sense of high vs low PEEP ventilation strategies.
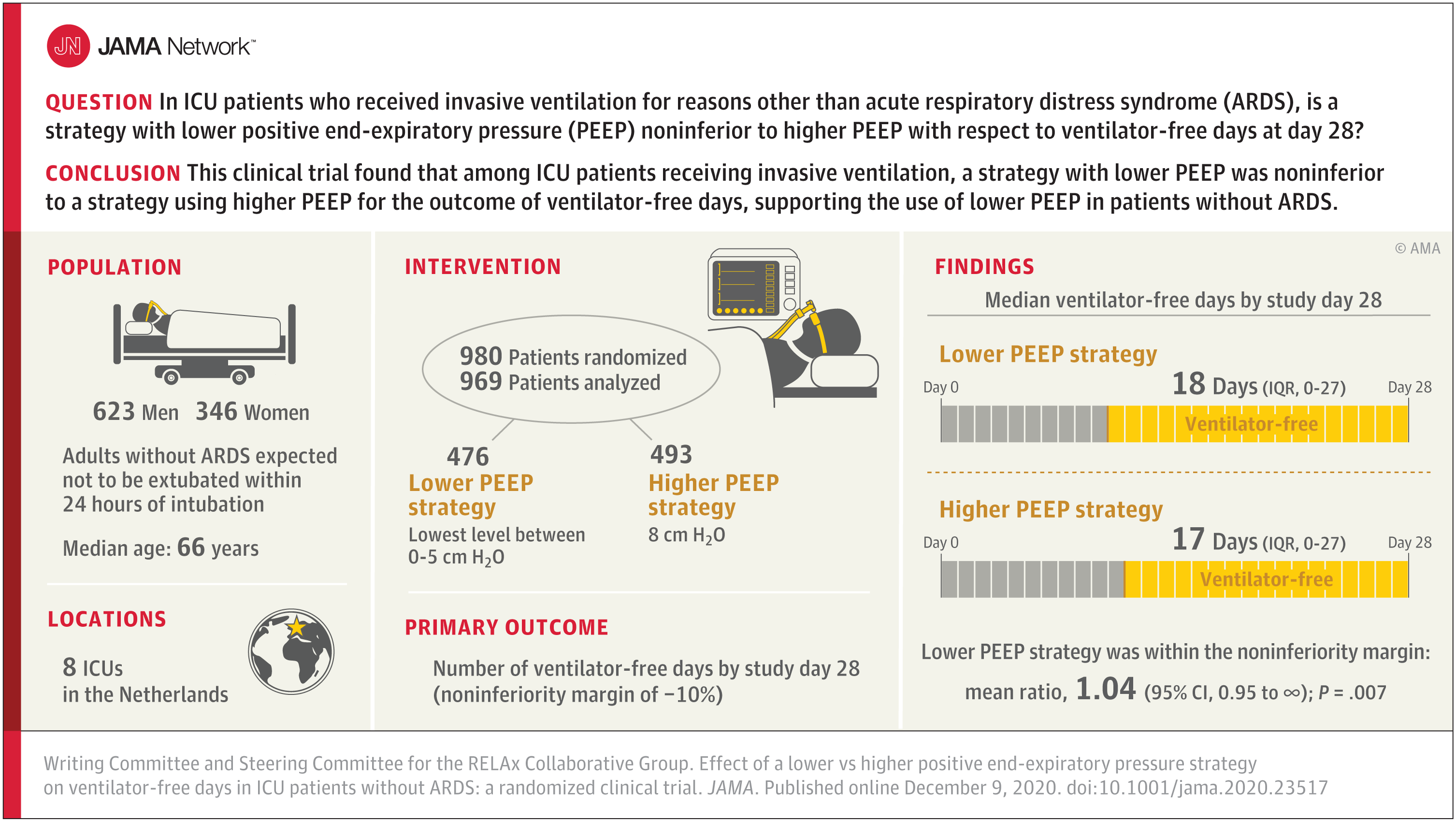
This noninferiority trial compares the effects of lower (0-5 cm H2O) vs higher (8 cm H2O) positive end-expiratory pressure (PEEP) on ventilator-free days at day 28 among critically ill patients without acute respiratory distress syndrome (ARDS).

jamanetwork.com
From a practical management standpoint, I'll always favor a high PEEP strategy since if anything happens it's much easier to tell a nurse or RT to increase the FiO2 than it is to tell them to increase the PEEP.