You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
3D TEE
Started by confusingleaf

At the moment I think 3D's uses are pretty limited. I use it for measuring the AV annular area in 3D and getting a nice general sense of the MV pathology on MVRs. Sometimes it's useful to then use the 3D data set to get 2D "views" where you know exactly where your 2D plane is slicing.
The few resources I've found have generally been through pubmed searches with terms like "3D evaluation of mitral valve" or "aortic annulus," etc. There are a few expensive books out there that will be obsolete in a few years.
Here's one that looked good when I flipped through it, but didn't buy:
Amazon product ASIN 1451143222
The few resources I've found have generally been through pubmed searches with terms like "3D evaluation of mitral valve" or "aortic annulus," etc. There are a few expensive books out there that will be obsolete in a few years.
Here's one that looked good when I flipped through it, but didn't buy:
Amazon product ASIN 1451143222
Attachments
Not sure the link showed up. Can't figure it out now - but it's Comprehensive Atlas of 3D Echocardiography, by Stanton Shernan. Easy to find on Amazon.
It is very useful. Live 3D for image based guidance i.e. Transeptal puncture. MV anatomy. AV annulus. 3D EF (quantification guidelines) 3D planimetry for MS, 3D vena contracta/EROA for MR and TR. I anticipate new echo guidelines for valve quantification in the coming years will recommend more 3D measurements. I haven't read that book by Shernan, but he did come and lecture to my echo group about a year ago for a whole weekend. Knows his stuff. Read the 3D echo guidelines as well. And just practice.
It is very useful. Live 3D for image based guidance i.e. Transeptal puncture. MV anatomy. AV annulus. 3D EF (quantification guidelines) 3D planimetry for MS, 3D vena contracta/EROA for MR and TR. I anticipate new echo guidelines for valve quantification in the coming years will recommend more 3D measurements. I haven't read that book by Shernan, but he did come and lecture to my echo group about a year ago for a whole weekend. Knows his stuff. Read the 3D echo guidelines as well. And just practice.
sorry--your first sentence says "it is very useful"--which resource ar eyou referring to? not the shernan book?
sorry--your first sentence says "it is very useful"--which resource ar eyou referring to? not the shernan book?
He is saying 3D is very useful
🙂
Here is a gold nugget for you.
These machines are very expensive as are the probes. First, don't get the GE 3D machine, I personally think it is a far cry from the Phillips i33 or the equally bada$$ Siemens 3d machine.


Now, since your department has purchased this machine, EVERY vendor will come out to your location and give you live tutorials... as in during a pump run or TAVR or if you do your own pre-op TEE's/cardioversions. The probes eventually break and to service them it can easily be 25k or more (I would engage in a service contract if I had the option). These vendors know the machine very, very well and are happy to fly out to your site.
Anyone have good resources for teaching yourself 3D TEE?
seems like at recent meeting all are signalling the death knell of 2D, though i think that's extreme.
helps to have a good machine. we have two, and one freezes every time you try to do 3D
Here is a gold nugget for you.
These machines are very expensive as are the probes. First, don't get the GE 3D machine, I personally think it is a far cry from the Phillips i33 or the equally bada$$ Siemens 3d machine.
Now, since your department has purchased this machine, EVERY vendor will come out to your location and give you live tutorials... as in during a pump run or TAVR or if you do your own pre-op TEE's/cardioversions. The probes eventually break and to service them it can easily be 25k or more (I would engage in a service contract if I had the option). These vendors know the machine very, very well and are happy to fly out to your site.
2D, PWD, CWD, TDI, etc isn't going anywhere, but 3D TEE is absolutely amazing. The level of interrogation is ridiculous. It is the next step in evolution of echocardiography. Here are a couple from last week. How often do you see the 3 struts of a bioprosthetic valve? Echocardiography has come a long way, and I am very happy that anesthesiologists have owned this advancement in medicine.


Awesome images, Sevo.
OP, if you have a Philips machine, you can ask one of their reps about going to one of their 3D TEE courses. When we bought our current i33 and probe several years ago, we were given several education credits to use for their courses. I went to their 3D TEE in Structural Heart Disease course last year, and it was pretty good. None of my current partners do 3D, so talking to others at the course was one of the only ways I had to figure out how to properly do 3D on our machine.
OP, if you have a Philips machine, you can ask one of their reps about going to one of their 3D TEE courses. When we bought our current i33 and probe several years ago, we were given several education credits to use for their courses. I went to their 3D TEE in Structural Heart Disease course last year, and it was pretty good. None of my current partners do 3D, so talking to others at the course was one of the only ways I had to figure out how to properly do 3D on our machine.
And what do I do now with this remarkable finding of a prostethic valve having 3 struts?2D, PWD, CWD, TDI, etc isn't going anywhere, but 3D TEE is absolutely amazing. The level of interrogation is ridiculous. It is the next step in evolution of echocardiography. Here are a couple from last week. How often do you see the 3 struts of a bioprosthetic valve? Echocardiography has come a long way, and I am very happy that anesthesiologists have owned this advancement in medicine.
I'll take the contrarian side and argue that 3d does not provide any new meaningful data over 2d. Maybe helps measuring the aortic annulus but I don't see it is big deal by it self. Surgeon will size them with a sizer, and the tavrs get ct scan measurements.
Last edited:
Advertisement - Members don't see this ad
this is a bit how i feel--they are awesome, fancy images and a 3D of the mitral is genuinely useful in determining the pathology. i also like a full volume with color to evaluate for paravalvular leaks after pump. this is about the level of my skill. and i will go into the future and try to teach myself the rest but i don't see how it changes my practice CLINICALLY. i can do the dancing jellybean of the LV but is that going to change the surgery being performed or the outcome post pump?
I get 3d of the mitral because it gets "ooohhsss and "aaahhhss", but when I want to pinpoint where the pathology is I do it in 2d. 3d can be decieving.this is a bit how i feel--they are awesome, fancy images and a 3D of the mitral is genuinely useful in determining the pathology. i also like a full volume with color to evaluate for paravalvular leaks after pump. this is about the level of my skill. and i will go into the future and try to teach myself the rest but i don't see how it changes my practice CLINICALLY. i can do the dancing jellybean of the LV but is that going to change the surgery being performed or the outcome post pump?
I don't find 3D all that useful yet. However, the modeling software is getting better and better. I think within the next 10 years or so you'll be able to push a button or 2 and have a nice 3D model of LV function and possibly even RV function. Same with the mitral valve. Reducing variability between examiners will be 3d's true value.
3D tee isn't replacing 2D, it is an adjunct. Let's get that straight.
So, I did 3 TAVRS a couple of days ago. One came down with a $hitty CT and poor contrast due to morbid obesity and abdominal breathing during the CT scan. Rep wasn't sure, but thought that a 29mm was the right size. Measured it in 3D and it mesured a solid 26mm. Deployed it and zero leak. How much do these valves cost? 35k?
Picked up on a small dehiscence that wan't extremely evident on 2d. No question with the 3d images and I could tell the surgeon exactly where to look when we went back on pump.
Percutaneous left atrial appendage closures. Measuring orifice area and appendage depth is useful.
Had a redo sternotomy for a 6 year old bioprosthetic valve/neo aorta that had torrential AI recently. Calcifications were so impressive that it was hard to see the aortic leaflets. Looked at it in 3d and guess what... the leaflets were completely gone and very obvious on the 3d aquisition (calcifications actually can help with 3d image acquisitions). The 3D pic was exactly what it looked like when we opened up the heart and looked at the aortic valve.
I find that looking at a1,a2,a3 and p1,p2,p3 is a lot cleaner on 3d. Sure, 2d gives the same info, but not the level of detail IMO. Both of them together increases the power of the exam.
So I'm not here to argue weather it has value or not. I personally find it very valuable. 90% of my images are 2D, but 3D has a wealth of information to be gathered in the right case/circumstances.
Furthermore, we don't know if any future procedures may need the guidance of 3D echocardiography. Being facile at it now certainly ins't a detriment to your exam.
Plus... it's a ton of fun to use. So what's the downside?
So, I did 3 TAVRS a couple of days ago. One came down with a $hitty CT and poor contrast due to morbid obesity and abdominal breathing during the CT scan. Rep wasn't sure, but thought that a 29mm was the right size. Measured it in 3D and it mesured a solid 26mm. Deployed it and zero leak. How much do these valves cost? 35k?
Picked up on a small dehiscence that wan't extremely evident on 2d. No question with the 3d images and I could tell the surgeon exactly where to look when we went back on pump.
Percutaneous left atrial appendage closures. Measuring orifice area and appendage depth is useful.
Had a redo sternotomy for a 6 year old bioprosthetic valve/neo aorta that had torrential AI recently. Calcifications were so impressive that it was hard to see the aortic leaflets. Looked at it in 3d and guess what... the leaflets were completely gone and very obvious on the 3d aquisition (calcifications actually can help with 3d image acquisitions). The 3D pic was exactly what it looked like when we opened up the heart and looked at the aortic valve.
I find that looking at a1,a2,a3 and p1,p2,p3 is a lot cleaner on 3d. Sure, 2d gives the same info, but not the level of detail IMO. Both of them together increases the power of the exam.
So I'm not here to argue weather it has value or not. I personally find it very valuable. 90% of my images are 2D, but 3D has a wealth of information to be gathered in the right case/circumstances.
Furthermore, we don't know if any future procedures may need the guidance of 3D echocardiography. Being facile at it now certainly ins't a detriment to your exam.
Plus... it's a ton of fun to use. So what's the downside?
Ohhh... my first day in the OR with a valve specialist (that's all he does....) His first question to me what was as follows:
"Can you show me a 3d view of the tricuspid valve?"
True story.
"Can you show me a 3d view of the tricuspid valve?"
True story.
****! i don't know that i've ever actually tried to 3D the tricuspid valve, but i'm sure it's more challenging than i can imagine.Ohhh... my first day in the OR with a valve specialist (that's all he does....) His first question to me what was as follows:
"Can you show me a 3d view of the tricuspid valve?"
True story.
i don't disagree with you that it has its place. but at recent conferences, i'm getting the impression that the "big guys" are doing all their 3D imaging first, and extensive 3D imaging and leaving 2D to pick up the pieces. i think it's a good adjunct, and maybe i'm just not there yet with my 3D skill but i can't imagine basically forgoing my 2D images
They need to constantly come up with new stuff, whether it is helpful or not. Otherwise people will stop going to the meetings. They depend on the vendors to make these meetings profitable also. There will always be something they focus on. Seems like diastology has been relegated to 2nd or 3rd place.****! i don't know that i've ever actually tried to 3D the tricuspid valve, but i'm sure it's more challenging than i can imagine.
i don't disagree with you that it has its place. but at recent conferences, i'm getting the impression that the "big guys" are doing all their 3D imaging first, and extensive 3D imaging and leaving 2D to pick up the pieces. i think it's a good adjunct, and maybe i'm just not there yet with my 3D skill but i can't imagine basically forgoing my 2D images
Last edited:
Maybe the point that they were trying to make regarding getting 3D images first is that once the surgeons start using the bovie, that will introduce interference and stitch artifact with 3D images, significantly worsening quality moreso than with 2D images. The 2D loops can be obtained in the seconds between bovie bursts.
Or, maybe Urge is correct, and this is just the latest new thing they wish to harp on in order to sell lectures.
Or, maybe Urge is correct, and this is just the latest new thing they wish to harp on in order to sell lectures.
****! i don't know that i've ever actually tried to 3D the tricuspid valve, but i'm sure it's more challenging than i can imagine.
i don't disagree with you that it has its place. but at recent conferences, i'm getting the impression that the "big guys" are doing all their 3D imaging first, and extensive 3D imaging and leaving 2D to pick up the pieces. i think it's a good adjunct, and maybe i'm just not there yet with my 3D skill but i can't imagine basically forgoing my 2D images
I'm with you. 👍
2D isn't going anywhere. It's here to stay. Heck I still use M-mode. I find it useful in a lot of circumstances.
There is just structures you can't see on a 2D exam that you can see in a 3D exam. Looking at the tricuspid valve from the RA and RV side can't be done with 2D- period! I don't care how good your 2d view of a tricuspid valve is.
Does it make a difference always? NO.
Sometimes? DEFINATELY.
So... why not learn this technology and use it to the benefit of your patients?

(from last week)
@ confusingleaf
Here are just a couple I quickly found. There are lots of them out there. Some in some really cool places. You'll get CME and focus entirely on 3D TEE.
http://www.unmc.edu/anesthesia/echo/3d/index.html
http://www.learningconnection.philips.com/zh-hans/course/advanced-live-intraoperative-3d-tee
Here are just a couple I quickly found. There are lots of them out there. Some in some really cool places. You'll get CME and focus entirely on 3D TEE.
http://www.unmc.edu/anesthesia/echo/3d/index.html
http://www.learningconnection.philips.com/zh-hans/course/advanced-live-intraoperative-3d-tee
Advertisement - Members don't see this ad
@ confusingleaf
Here are just a couple I quickly found. There are lots of them out there. Some in some really cool places. You'll get CME and focus entirely on 3D TEE.
http://www.unmc.edu/anesthesia/echo/3d/index.html
http://www.learningconnection.philips.com/zh-hans/course/advanced-live-intraoperative-3d-tee
thank you much! appreciate your help and knowledge.
I'm with you. 👍
2D isn't going anywhere. It's here to stay. Heck I still use M-mode. I find it useful in a lot of circumstances.
There is just structures you can't see on a 2D exam that you can see in a 3D exam. Looking at the tricuspid valve from the RA and RV side can't be done with 2D- period! I don't care how good your 2d view of a tricuspid valve is.
Does it make a difference always? NO.
Sometimes? DEFINATELY.
So... why not learn this technology and use it to the benefit of your patients?
(from last week)
oh--may i ask how you got a good tricuspid view? 3D zoom from RV in flow outflow? or did you crop a full volume
There is no denying that these are beautiful pictures of the valves. But, what do you do with them?I'm with you. 👍
2D isn't going anywhere. It's here to stay. Heck I still use M-mode. I find it useful in a lot of circumstances.
There is just structures you can't see on a 2D exam that you can see in a 3D exam. Looking at the tricuspid valve from the RA and RV side can't be done with 2D- period! I don't care how good your 2d view of a tricuspid valve is.
Does it make a difference always? NO.
Sometimes? DEFINATELY.
So... why not learn this technology and use it to the benefit of your patients?
(from last week)
I think 3D/color 3D is good for a few things. By far the biggest utility is in mitral repair, where it is indispensable.
But for the most part, I think the purpose of 3D is to demonstrate to those around you that you're a competent echocardiographer.
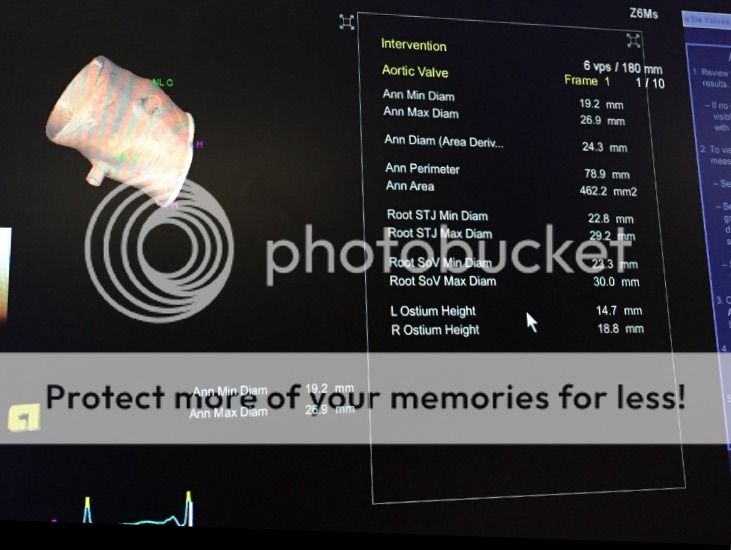
I don't find much utility in aortic valve surgery TBH. I use it to get an accurate 3D planimetry of the LVOT area, just to reduce the squared error in the 2D method, but it's not like that is an earth-shattering difference.
But for the most part, I think the purpose of 3D is to demonstrate to those around you that you're a competent echocardiographer.
I don't find much utility in aortic valve surgery TBH. I use it to get an accurate 3D planimetry of the LVOT area, just to reduce the squared error in the 2D method, but it's not like that is an earth-shattering difference.
There is no denying that these are beautiful pictures of the valves. But, what do you do with them?

I'll stick by my assertion that 3d is an amazing tool and that combined with 2d, you get a study that has significant power.
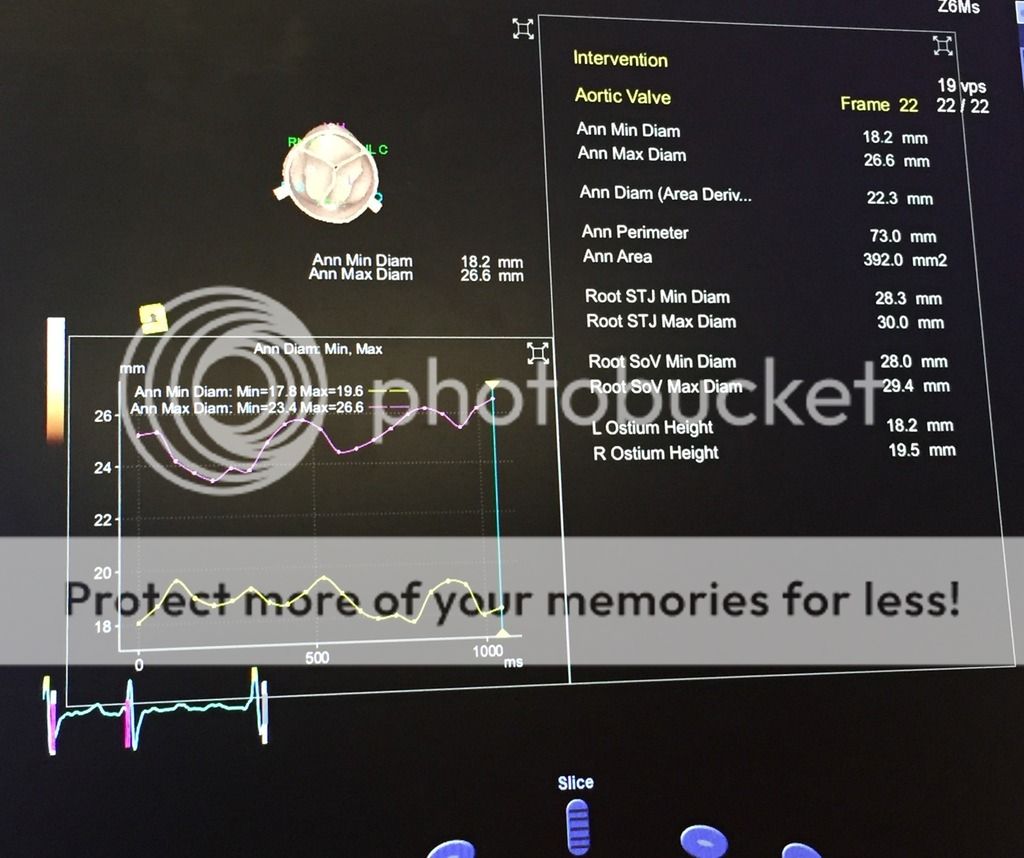
More so with 3d as you can take several clips with thousands of data points and analyze that data pre, intra or post op with some pretty amazing software.
I think that the source of error is vastly diminished.
Looking at things from different aspects doesn't have a down side.
Valves, tumors, shunts, interventions, funny looking stuff you are not exactly sure of.
What am I looking at here?
You ever see something on a valve that might look like a vegetation or might look like a calcium deposit? I find 3d helpful in these situations.
It's not useless technology and accurate data can be obtained remarkably quickly.
Valves, tumors, shunts, interventions, funny looking stuff you are not exactly sure of.
What am I looking at here?
You ever see something on a valve that might look like a vegetation or might look like a calcium deposit? I find 3d helpful in these situations.
It's not useless technology and accurate data can be obtained remarkably quickly.
VHS is good but I prefer a blue ray disk when I have the option. 🙂
And what exactly do I do with this information?
I'll stick by my assertion that 3d is an amazing tool and that combined with 2d, you get a study that has significant power.
More so with 3d as you can take several clips with thousands of data points and analyze that data pre, intra or post op with some pretty amazing software.
I think that the source of error is vastly diminished.
You know... stuff like:
Hey the left coronary ostial height is only 6mm and risk of coronary obstruction is high. Please keep that in mind before you deploy your sapien 3 valve.
Or...
Your suboptimal CT measurement of the aortic ann. area was 490mm, but I am confident it's around 615mm.
You might consider a 16 sheath instead of a 14 in this patient as a 14 sheath might not accommodate a 29mm valve.
Or...
You show up for a minimally invasive MVR and your surgeon asks you for the intertrigonal and intercommissural distance before we get started.
You know... stuff like that.
3D increases the power of my decision making.
Hey the left coronary ostial height is only 6mm and risk of coronary obstruction is high. Please keep that in mind before you deploy your sapien 3 valve.
Or...
Your suboptimal CT measurement of the aortic ann. area was 490mm, but I am confident it's around 615mm.
You might consider a 16 sheath instead of a 14 in this patient as a 14 sheath might not accommodate a 29mm valve.
Or...
You show up for a minimally invasive MVR and your surgeon asks you for the intertrigonal and intercommissural distance before we get started.
You know... stuff like that.
3D increases the power of my decision making.