that's great and all but the question is how are they doing iti haven't met a dermatologist that does not see less than 50 per day, they get worried when there is less than 50 on the schedule
I know one particular spine surgeon that sees 60 patients per day in his office day. He laughed at me when I told him I usually see 20 to 25
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
40-50 patients a day. How?
- Thread starter agolden1
- Start date

the point was that a lot of docs and different specialties do it...Ithat's great and all but the question is how are they doing it
In and out of the room in 5min. the spine surgeon has a PA that does all the notes for him
- Joined
- Jun 16, 2012
- Messages
- 324
- Reaction score
- 116
My friend, 99.2, 99.6, 99.8 percentile will be a huge difference, to this extreme, people can make a few more millions, with 0.5% difference.If you're seeing 40-50 pts per day in an ortho clinic...Not a traditional pain clinic...An ortho clinic.
You're 99th percentile.
The vast majority of pts will be procedural candidates, and there will be less fibro and other BS diagnoses leading nowhere.
")
- Joined
- Aug 16, 2007
- Messages
- 5,385
- Reaction score
- 2,526
Well as someone looking for a home I think home prices have been grossly inflated these last couple of years. A house that cost $600k pre pandemic is now $900k. Same damn house. It’s annoying. Real estate agents are incentivized to sell. I don’t think they’re too incentivized to help the buyer. And it’s the easiest job around. They have a program that writes up the contract in 3 min. Making 3% on 1 million. That’s a quick 30k. My realtor personally sold 44 million last yearInteresting analogy btw. What'd you mean by the RE agent COVID relationship?
I think the whole agent broker setup in general is a scam also.
- Joined
- Mar 31, 2008
- Messages
- 1,384
- Reaction score
- 2,034
Ophto's and vascular surgeons also easily churn through 50 per dayi haven't met a dermatologist that does not see less than 50 per day, they get worried when there is less than 50 on the schedule
I know one particular spine surgeon that sees 60 patients per day in his office day. He laughed at me when I told him I usually see 20 to 25
dang, problem is the average realtor doesn't make much - but the top1% make millions and even have their own reality tv showsWell as someone looking for a home I think home prices have been grossly inflated these last couple of years. A house that cost $600k pre pandemic is now $900k. Same damn house. It’s annoying. Real estate agents are incentivized to sell. I don’t think they’re too incentivized to help the buyer. And it’s the easiest job around. They have a program that writes up the contract in 3 min. Making 3% on 1 million. That’s a quick 30k. My realtor personally sold 44 million last year
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
imo, the reason all of the work we do is devalued is because of these doctors seeing 40-50 patients a day. this is assembly line work and pretty worthless.
we should view medical care and what we do more like baristas who spend time and effort to make the perfect doppio, than a soda machine that pours out liquid garbage.
we should view medical care and what we do more like baristas who spend time and effort to make the perfect doppio, than a soda machine that pours out liquid garbage.
- Joined
- Apr 28, 2010
- Messages
- 1,313
- Reaction score
- 1,385
We do. Unfortunately, payers want to buy a doppio for the price of a sodawe should view medical care and what we do more like baristas who spend time and effort to make the perfect doppio, than a soda machine that pours out liquid garbage.
- Joined
- May 26, 2010
- Messages
- 3,526
- Reaction score
- 2,078
You're right. It's a racket. You can always consider getting your real estate license and being your own agent to keep that commission. That's what we did. You can also refer your friends to realtors and get 25% of the commission of one side. Then give your friend half.Well as someone looking for a home I think home prices have been grossly inflated these last couple of years. A house that cost $600k pre pandemic is now $900k. Same damn house. It’s annoying. Real estate agents are incentivized to sell. I don’t think they’re too incentivized to help the buyer. And it’s the easiest job around. They have a program that writes up the contract in 3 min. Making 3% on 1 million. That’s a quick 30k. My realtor personally sold 44 million last year
- Joined
- Aug 28, 2019
- Messages
- 85
- Reaction score
- 159
There are a lot of reasons doctors choose to see 40-50 patients per day. $$$, some like that pace, volume of referrals, maturity of practice.
I wouldn't want to be the 45th patient on a 50 patient schedule. And I wouldn't want that for my wife or children either. Of course, no one asks the patient how they feel about it.
I wouldn't want to be the 45th patient on a 50 patient schedule. And I wouldn't want that for my wife or children either. Of course, no one asks the patient how they feel about it.
- Joined
- May 5, 2013
- Messages
- 267
- Reaction score
- 179
i haven't met a dermatologist that does not see less than 50 per day, they get worried when there is less than 50 on the schedule
I know one particular spine surgeon that sees 60 patients per day in his office day. He laughed at me when I told him I usually see 20 to 25
Having family and friends in Derm and Ophtho, I get how they can accomplish this in a well oiled machine. Scribes enter in everything, they never touch a computer or a note aside from signing at days end. I've often wondered how the fields evolved so differently to rely on scribes (derm ophtho) vs to rely so heavily on dictation/self entry (pain). General overhead of the group I suppose.
I worry for the patient of a spine surgeon who sees 60 patients a day. I can't imagine making the decision for a fusion based on a five minute interaction, but maybe they're seeing things faster than I am in terms of "surgery, no surgery."
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
I worry for the patient of a spine surgeon who sees 60 patients a day. I can't imagine making the decision for a fusion based on a five minute interaction, but maybe they're seeing things faster than I am in terms of "surgery, no surgery."
edited it for you:
D
deleted875186
I suspect they’re recommending surgery based on the business of their OR schedule. Have someone in my area that does ALIF and posterior fusion at once all the time for single level disc herniation. I often wonder how the conversation in the neurosurgery clinic went.Having family and friends in Derm and Ophtho, I get how they can accomplish this in a well oiled machine. Scribes enter in everything, they never touch a computer or a note aside from signing at days end. I've often wondered how the fields evolved so differently to rely on scribes (derm ophtho) vs to rely so heavily on dictation/self entry (pain). General overhead of the group I suppose.
I worry for the patient of a spine surgeon who sees 60 patients a day. I can't imagine making the decision for a fusion based on a five minute interaction, but maybe they're seeing things faster than I am in terms of "surgery, no surgery."
and when it doesn't work, they can't do anything else and you must go to pain management.I suspect they’re recommending surgery based on the business of their OR schedule. Have someone in my area that does ALIF and posterior fusion at once all the time for single level disc herniation. I often wonder how the conversation in the neurosurgery clinic went.
it's really a great business model for them
- Joined
- Jun 16, 2012
- Messages
- 324
- Reaction score
- 116
This is just my observation, 40-50 patients per day in a well organized orthopedics group is achievable, and have good satisfaction from patients, this is across subspecialties hands, shoulder, sports, reconstructions and spine, however some surgeon sees 60-100 cases a day, this is over too much to me, he is just in and out in couple minutes .
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
ive been in doctors offices in which the appointments are 5-8 minutes. its laughable to think that patients are really that satisfied when the doctor flies in and out without the door ever closing behind them.
but i do admit, 8 minutes is a lot better than 2.
but i do admit, 8 minutes is a lot better than 2.
- Joined
- Jun 16, 2012
- Messages
- 324
- Reaction score
- 116
i agree, however, patient's satisfaction is affected by many factors, including community standards, specialty difference, well designed clinical setting, also supporting staff like MA, PA and NPs, most of history, exam are done, only further discussion.ive been in doctors offices in which the appointments are 5-8 minutes. its laughable to think that patients are really that satisfied when the doctor flies in and out without the door ever closing behind them.
but i do admit, 8 minutes is a lot better than 2.
- Joined
- Aug 5, 2011
- Messages
- 528
- Reaction score
- 398
So how would the future of value-based reimbursement affect high volume practices if fee-for-service goes away in the future? Or is it a fallacy that more time you spend with a patient provides better care
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
Competent doctors provide high level care regardless of time spent in front of a pt.
I would consider it may be true the longer you spend in the exam room the more likely you are to harm that pt. Same holds true for spending minimal time with that pt.
Patient population matters. Medicaid pts take longer in the clinic and are far more likely to have negative outcomes.
I would consider it may be true the longer you spend in the exam room the more likely you are to harm that pt. Same holds true for spending minimal time with that pt.
Patient population matters. Medicaid pts take longer in the clinic and are far more likely to have negative outcomes.
- Joined
- May 25, 2011
- Messages
- 148
- Reaction score
- 135
Competent doctors provide high level care regardless of time spent in front of a pt.
I would consider it may be true the longer you spend in the exam room the more likely you are to harm that pt. Same holds true for spending minimal time with that pt.
Patient population matters. Medicaid pts take longer in the clinic and are far more likely to have negative outcomes.
“I would consider it may be true the longer you spend in the exam room the more likely you are to harm that pt.”
Can you explain more what you mean by this?
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
If you're in an exam room longer than 20 min you're floundering. You either don't know what to do or you're bargaining.“I would consider it may be true the longer you spend in the exam room the more likely you are to harm that pt.”
Can you explain more what you mean by this?
There's a sweet spot of around 10-15 min where you're examining the pt, getting an HPI, formulating and explaining a plan.
A 3 min visit prob means you did not touch the pt and most likely the pt doesn't understand the plan or their imaging. That pt is more likely than not ignorant of their situation and what's going on...
The greater the face time the greater the odds you are furthering care with new medications and repeated procedures.
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
not sure where you got the idea that spending more time with the patient is harmful.Competent doctors provide high level care regardless of time spent in front of a pt.
I would consider it may be true the longer you spend in the exam room the more likely you are to harm that pt. Same holds true for spending minimal time with that pt.
Patient population matters. Medicaid pts take longer in the clinic and are far more likely to have negative outcomes.
more time leads to more education and more discussion on lifestyle changes.
i found no study that shows that longer time spent causes harm. but i also did not find any study so far that shows that longer time definitively equates to better care. that is partly because of how hard it is to define better care.
i did find studies that show that shorter times leads to poorer doctor-patient communication and poorer relationship and increased level of patient frustration with medical care.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
More time with a pt results in more care provided.not sure where you got the idea that spending more time with the patient is harmful.
more time leads to more education and more discussion on lifestyle changes.
I don't need a study to tell me that, just like I don't need a study to tell me using a parachute saves lives when jumping out of an airplane.
- Joined
- May 30, 2005
- Messages
- 21,257
- Reaction score
- 12,372
Sometimes the Ortho rubs off on the PMR guy who works for Ortho. see above post.
I think he meant to say that longer visits can be a symptom rather than a cause of suboptimal care.
ie: Someone is inefficient because they can't clearly formulate a treatment plan or evaluate their patient in an organized matter, thereby wasting time.
The way I see it, if you take 50% more time to offer care of an equivalent quality, you're possibly doing something wrong. If you taking more time allows you to add value, all is fine.
ie: Someone is inefficient because they can't clearly formulate a treatment plan or evaluate their patient in an organized matter, thereby wasting time.
The way I see it, if you take 50% more time to offer care of an equivalent quality, you're possibly doing something wrong. If you taking more time allows you to add value, all is fine.
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
and how exactly is more care harmful?More time with a pt results in more care provided.
I don't need a study to tell me that, just like I don't need a study to tell me using a parachute saves lives when jumping out of an airplane.
what i did learn from the studies i saw is that much more lifestyle changes is provided with longer times spent with patient. not sure how this is harmful, and you are making an assumption that because you spend longer with a patient you are more likely to order an injection or a med? i find that specious.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
Incorrect.Sometimes the Ortho rubs off on the PMR guy who works for Ortho. see above post.
After a debatable amount of time, you're either spinning your wheels in the mud or pulling things out of your behind. If you can't get through to that pt after x minutes, you're screwed.
The more ignorant your pt, the more likely they'll fail your treatment, the less likely they'll understand what is going on during an MBB, etc.
Seriously dude?and how exactly is more care harmful?
You're right...There's no added harm in adding another few medications or repeating more shots or getting new imaging.
The longer your face time with that pt the more likely you're going to do one of those things.
- Joined
- Apr 13, 2016
- Messages
- 2,665
- Reaction score
- 2,640
I see where you’re coming from but it doesn’t apply across the board. I have lots of patients who come from 2-3 hours away, so when I see them for their back, and their neck is also hurting, and they’ve got a bad knee, and they’ve got carpal tunnel, I have a bad habit of getting sucked into addressing all those in one visit.Incorrect.
After a debatable amount of time, you're either spinning your wheels in the mud or pulling things out of your behind. If you can't get through to that pt after x minutes, you're screwed.
The more ignorant your pt, the more likely they'll fail your treatment, the less likely they'll understand what is going on during an MBB, etc.
Seriously dude?
You're right...There's no added harm in adding another few medications or repeating more shots or getting new imaging.
The longer your face time with that pt the more likely you're going to do one of those things.
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
please prove that spending more time results in more medications.
it is much easier to throw meds at a patient as you are running out of the room to get to your next patient than if you are sitting down with the patient and discussing things such as exercise, weight loss, core strengthening, changes in lifestyle.
if you feel that you have to throw meds or shots or injections at a patient because you spend more time with them - well, that is on you.
===
this study suggests that later in the day and physicians being behind - and that can happen with shorter times with patients and higher volumes - leads to increased opioid prescribing.
 www.inverse.com
www.inverse.com
the actual study:

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
===
here is a study that shows that under time pressure, physicians are less likely to adhere to guidelines and give less lifestyle choices.
its easy to write a script or order a test and get out the door.
it is much easier to throw meds at a patient as you are running out of the room to get to your next patient than if you are sitting down with the patient and discussing things such as exercise, weight loss, core strengthening, changes in lifestyle.
if you feel that you have to throw meds or shots or injections at a patient because you spend more time with them - well, that is on you.
===
this study suggests that later in the day and physicians being behind - and that can happen with shorter times with patients and higher volumes - leads to increased opioid prescribing.
2 Time Factors Increase the Chances Your Doctor Will Prescribe Opioids
Doctors get worn out, just like the rest of us.
The data revealed that as the day progressed, doctors became 33 percent more likely to write opioid prescriptions for patients who were in pain — from 4 percent during the first few appointments of the day to 5.3 percent for the last few of the day.
Additionally, the likelihood that doctors prescribed opioids also increased by 17 percent as they fell behind schedule. Chances of opioid prescriptions rose from a 4.4 percent chance when doctors were running less than 9 minutes behind schedule to a 5.2 percent chance when they were running an hour behind or more.
the actual study:
Association of Primary Care Clinic Appointment Time With Opioid Prescribing - PubMed
These findings suggest that, even within an individual physician's schedule, clinical decision-making for opioid prescribing varies by the timing and lateness of appointments.
pubmed.ncbi.nlm.nih.gov
===
here is a study that shows that under time pressure, physicians are less likely to adhere to guidelines and give less lifestyle choices.
its easy to write a script or order a test and get out the door.
i feel like the longer you're in the room, either 1)you got sucked into their never ending conversations and you don't know how to bail or 2) you're actually trying to educate patient . Never would I think long clinic visits are due to suboptimal care, but it certainly affects your bottom line.
- Joined
- Mar 31, 2008
- Messages
- 1,384
- Reaction score
- 2,034
Tbf, evidence doesn't show physicians are very effective at convincing patients to exercise, eat a healthier diet, or engage in lifestyle change regardless of time spent with patient.it is much easier to throw meds at a patient as you are running out of the room to get to your next patient than if you are sitting down with the patient and discussing things such as exercise, weight loss, core strengthening, changes in lifestyle.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
I won't treat all those in one visit, nor should you IMO. How can you educate them about 4 separate body parts in one visit? They're not going to remember all of that.I see where you’re coming from but it doesn’t apply across the board. I have lots of patients who come from 2-3 hours away, so when I see them for their back, and their neck is also hurting, and they’ve got a bad knee, and they’ve got carpal tunnel, I have a bad habit of getting sucked into addressing all those in one visit.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
i feel like the longer you're in the room, either 1)you got sucked into their never ending conversations and you don't know how to bail or 2) you're actually trying to educate patient . Never would I think long clinic visits are due to suboptimal care, but it certainly affects your bottom line.
How long does it take you to educate a pt?
Pt comes in with mild to moderate spinal stenosis and complains of back, buttock and leg pain.
How long do you think it takes to educate that pt?
- Joined
- May 30, 2005
- Messages
- 21,257
- Reaction score
- 12,372
Ornery. You are a physiatrist but sound like an Ortho “ bone break me fix it” guy.Incorrect.
After a debatable amount of time, you're either spinning your wheels in the mud or pulling things out of your behind. If you can't get through to that pt after x minutes, you're screwed.
The more ignorant your pt, the more likely they'll fail your treatment, the less likely they'll understand what is going on during an MBB, etc.
Seriously dude?
You're right...There's no added harm in adding another few medications or repeating more shots or getting new imaging.
The longer your face time with that pt the more likely you're going to do one of those things.

Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials
Objectives To determine whether parachutes are effective in preventing major trauma related to gravitational challenge.Design Systematic review of randomised controlled trials.Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; ...
 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
https://www.bmj.com/content/bmj/363/bmj.k5094.full.pdf
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
Do you ever actually read what other ppl post, or do you reflexively vomit links trying to make your point? I said, in my very first post on the matter that short visits and very long visits lead to worse outcomes.please prove that spending more time results in more medications.
it is much easier to throw meds at a patient as you are running out of the room to get to your next patient than if you are sitting down with the patient and discussing things such as exercise, weight loss, core strengthening, changes in lifestyle.
if you feel that you have to throw meds or shots or injections at a patient because you spend more time with them - well, that is on you.
===
this study suggests that later in the day and physicians being behind - and that can happen with shorter times with patients and higher volumes - leads to increased opioid prescribing.
2 Time Factors Increase the Chances Your Doctor Will Prescribe Opioids
Doctors get worn out, just like the rest of us.
the actual study:
Association of Primary Care Clinic Appointment Time With Opioid Prescribing - PubMed
These findings suggest that, even within an individual physician's schedule, clinical decision-making for opioid prescribing varies by the timing and lateness of appointments.
===
here is a study that shows that under time pressure, physicians are less likely to adhere to guidelines and give less lifestyle choices.
its easy to write a script or order a test and get out the door.
You just posted links (that I didn't read) agreeing with me, so I'm happy to say we agree that spending minimal time with a pt increases the likelihood your care sucks.
Long pt visits - There is a length of time after which care surely suffers. If you cannot get through to a pt in a reasonable amount of time (length is debatable as I've said), that pt is either intellectually challenged (outcomes suffer), you don't know what you're doing (outcomes suffer), you're stuck with a pt who's all over the place and bombarding you with 50 problems (outcomes suffer), you've got a difficult spouse (outcomes suffer), etc...
The longer you're in front if that pt, and the longer they have your ears the more likely some of them will pressure you for any number of things.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
You got me. I was reading that and they cleverly dropped that image at the end.Ornery. You are a physiatrist but sound like an Ortho “ bone break me fix it” guy.
Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials
Objectives To determine whether parachutes are effective in preventing major trauma related to gravitational challenge.Design Systematic review of randomised controlled trials.Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; ...
https://www.bmj.com/content/bmj/363/bmj.k5094.full.pdf
First statement isn't accurate.
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
i am arguing that you stated long visits are more likely to harm patients - your exact quote - and your quote:
if you are going to make your statement as an extreme, like spending hours with a patient, it is a moot point and ridiculous. noone is going to be idiotic enough to spend hours with a patient (unless you are palliative care or a psychiatrist).
but for your average patient, spending more time - like 15 minutes, not hours - with them will not cause harm. it will not lead to more prescriptions. it will not lead to more injections. well, maybe if that doctor is incompetent.
it may lead to better communication, better doctor patient relationship, and hopefully to better discussion on lifestyle choices.
Seriously dude?
You're right...There's no added harm in adding another few medications or repeating more shots or getting new imaging.
The longer your face time with that pt the more likely you're going to do one of those things.
if you are going to make your statement as an extreme, like spending hours with a patient, it is a moot point and ridiculous. noone is going to be idiotic enough to spend hours with a patient (unless you are palliative care or a psychiatrist).
but for your average patient, spending more time - like 15 minutes, not hours - with them will not cause harm. it will not lead to more prescriptions. it will not lead to more injections. well, maybe if that doctor is incompetent.
it may lead to better communication, better doctor patient relationship, and hopefully to better discussion on lifestyle choices.
- Joined
- Dec 12, 2006
- Messages
- 2,983
- Reaction score
- 3,483
You beat me to it. One of my favorite articles.Ornery. You are a physiatrist but sound like an Ortho “ bone break me fix it” guy.
Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials
Objectives To determine whether parachutes are effective in preventing major trauma related to gravitational challenge.Design Systematic review of randomised controlled trials.Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; ...
https://www.bmj.com/content/bmj/363/bmj.k5094.full.pdf
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
Like I said, there's a sweet spot of around 10-15 min. Face-to-face over 20 min is either nonmedical general conversation, a confused doctor or a difficult patient.i am arguing that you stated long visits are more likely to harm patients - your exact quote - and your quote:
if you are going to make your statement as an extreme, like spending hours with a patient, it is a moot point and ridiculous. noone is going to be idiotic enough to spend hours with a patient (unless you are palliative care or a psychiatrist).
but for your average patient, spending more time - like 15 minutes, not hours - with them will not cause harm. it will not lead to more prescriptions. it will not lead to more injections. well, maybe if that doctor is incompetent.
it may lead to better communication, better doctor patient relationship, and hopefully to better discussion on lifestyle choices.
If it takes you 45 min to do a follow up, there's a serious problem in that room and many physicians will do whatever TH it takes to get out of there.
Since you mentioned 15 min, I'd just say I beat you to the punch.
- Joined
- Dec 6, 2012
- Messages
- 477
- Reaction score
- 544
I feel like if I address to many issues with a patient they have no concept of the plan.
“I wore the wrist splints at night for my back like you said, but my back still hurts”
“I wore the wrist splints at night for my back like you said, but my back still hurts”
there is a difference between a "pain" model and an "orthopedic" model
for the pain patient, there is a lot more hand holding, explanations, multimodal approach, etc. in the orthopedic model, it is more of a tough love approach.
im a big fan of the ortho model.
ran out of empathy in 2012, but i can still do the right thing for the patient
for the pain patient, there is a lot more hand holding, explanations, multimodal approach, etc. in the orthopedic model, it is more of a tough love approach.
im a big fan of the ortho model.
ran out of empathy in 2012, but i can still do the right thing for the patient

I like this reference for the trainees when talking about how we can sometimes be too educated or offer too much
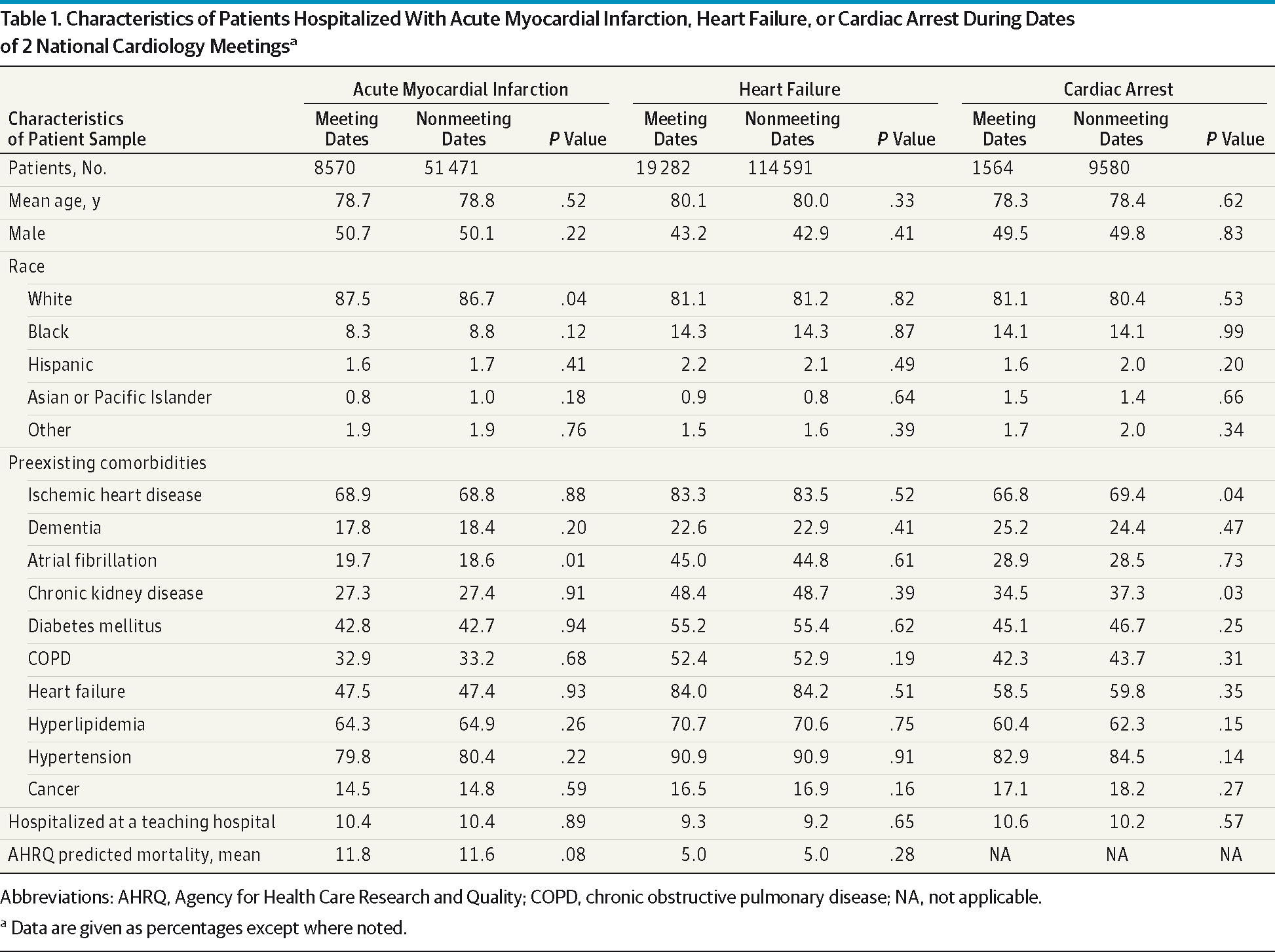
Mortality Patterns Among Patients With Acute Cardiovascular Conditions
High-risk patients with heart failure and cardiac arrest hospitalized in teaching hospitals had lower 30-day mortality when admitted during dates of national cardiology meetings. High-risk patients with acute myocardial infarction admitted to teaching hospitals during meetings were less likely to...
 jamanetwork.com
jamanetwork.com
Regarding the above reference for primary care, their later paper included this figure
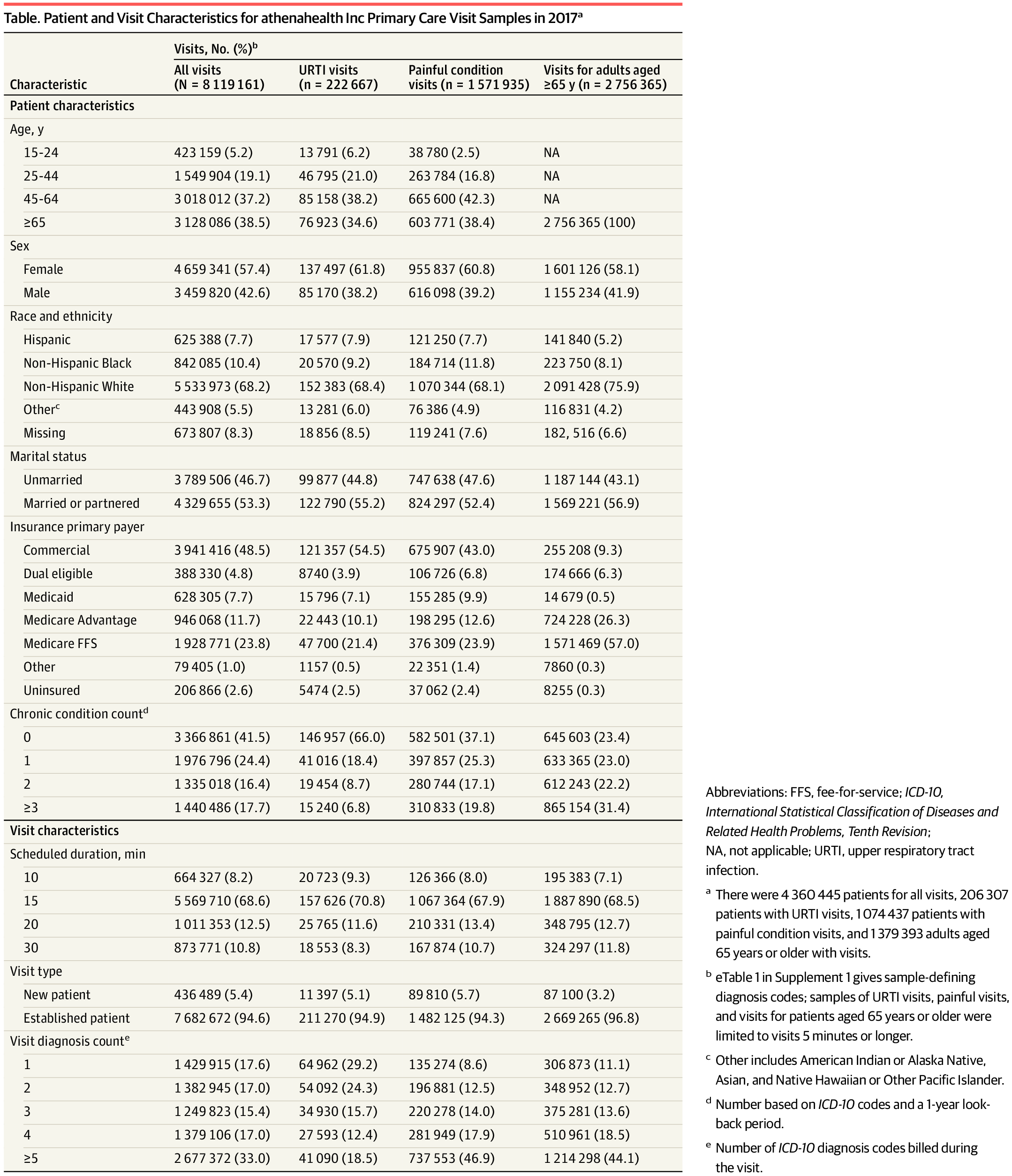
Association of Primary Care Visit Length With Potentially Inappropriate Prescribing
This cross-sectional study of a multistate sample of electronic health record data examines the association between primary care visit length and potentially inappropriate prescribing.
 jamanetwork.com
jamanetwork.com
A figure earlier in the that Neprash paper suggests most of what drives visit duration for primary care docs is the time allocated for the visit and the number of diagnoses treated. I would argue based off panel B though that inappropriate medication prescribing is more a function of provider factors than the visit duration.
I agree with @MitchLevi that if you are spending an inordinately long time with a patient that you're either attempting to be heroic or the patient is a trainwreck, and either way you'll likely end up with a worse outcome on average.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
The difference being Pain =/= Primary Care.
I like this reference for the trainees when talking about how we can sometimes be too educated or offer too much
"High-risk patients with heart failure and cardiac arrest hospitalized in teaching hospitals had lower 30-day mortality when admitted during dates of national cardiology meetings. High-risk patients with AMI admitted to teaching hospitals during meetings were less likely to receive PCI, without any mortality effect."Mortality Patterns Among Patients With Acute Cardiovascular Conditions
High-risk patients with heart failure and cardiac arrest hospitalized in teaching hospitals had lower 30-day mortality when admitted during dates of national cardiology meetings. High-risk patients with acute myocardial infarction admitted to teaching hospitals during meetings were less likely to...
Regarding the above reference for primary care, their later paper included this figure
View attachment 368549Association of Primary Care Visit Length With Potentially Inappropriate Prescribing
This cross-sectional study of a multistate sample of electronic health record data examines the association between primary care visit length and potentially inappropriate prescribing.
A figure earlier in the that Neprash paper suggests most of what drives visit duration for primary care docs is the time allocated for the visit and the number of diagnoses treated. I would argue based off panel B though that inappropriate medication prescribing is more a function of provider factors than the visit duration.
I agree with @MitchLevi that if you are spending an inordinately long time with a patient that you're either attempting to be heroic or the patient is a trainwreck, and either way you'll likely end up with a worse outcome on average.
- Joined
- Jun 23, 2012
- Messages
- 76
- Reaction score
- 26
What is everyone’s experience with scribes? I’m considering adding one as I’m now getting near 30 or more patients per day (new and follow ups) and notice I’m taking a large portion of work home with me. My concern is 1) will they be able to keep up with notes if I can’t? And 2) how hard is it train a scribe to really be useful and not a burden, i.e. re-reading the notes and adding changes. Also, have you all been successful in training staff to order and and provide patients with imaging studies, referrals, etc to make life easier on you? I still feel like I do a lot of the scut work.
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
meh. being a doctor is still being a doctor.The difference being Pain =/= Primary Care.
and remember that pain doctors are more likely to have discussions on potentially dangerous medications such as opioids than primary care.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
meh. being a doctor is still being a doctor.
Patient population matters.meh. being a doctor is still being a doctor.
and remember that pain doctors are more likely to have discussions on potentially dangerous medications such as opioids than primary care.
A PCP spending 30 min on a follow up isn't the same as a pain doctor doing a 30 min follow up.
There are many problems with a 30 min pain management follow up.
- Joined
- Apr 13, 2016
- Messages
- 2,665
- Reaction score
- 2,640
I have 2. They serve as both scribe and MA so they room the patient and out history into chart, then document my visit, enter orders, and complete the note. One is getting a patient ready while I’m in the other room. They do take a while to train up to where they save you time. I don’t see patients much faster (15 min f/u and 30 minute new) but I rarely work on notes at home.What is everyone’s experience with scribes? I’m considering adding one as I’m now getting near 30 or more patients per day (new and follow ups) and notice I’m taking a large portion of work home with me. My concern is 1) will they be able to keep up with notes if I can’t? And 2) how hard is it train a scribe to really be useful and not a burden, i.e. re-reading the notes and adding changes. Also, have you all been successful in training staff to order and and provide patients with imaging studies, referrals, etc to make life easier on you? I still feel like I do a lot of the scut work.
- Joined
- Jul 26, 2010
- Messages
- 2,349
- Reaction score
- 198
So I used to work at a hospital. We couldn't have nurses or MA order MRI etcI have 2. They serve as both scribe and MA so they room the patient and out history into chart, then document my visit, enter orders, and complete the note. One is getting a patient ready while I’m in the other room. They do take a while to train up to where they save you time. I don’t see patients much faster (15 min f/u and 30 minute new) but I rarely work on notes at home.
I like your idea of having a MA order meds or mri. How is tht done? Do they tee it up and ur signing it electronically make it "legal"?
- Joined
- Apr 13, 2016
- Messages
- 2,665
- Reaction score
- 2,640
Technically they are teeing up the order and I am signing the chart.So I used to work at a hospital. We couldn't have nurses or MA order MRI etc
I like your idea of having a MA order meds or mri. How is tht done? Do they tee it up and ur signing it electronically make it "legal"?
- Joined
- May 30, 2005
- Messages
- 21,257
- Reaction score
- 12,372
A doctor doing order entry or typing their own notes is a clerk.