
- Joined
- Aug 16, 2005
- Messages
- 110
- Reaction score
- 80
Hi all,
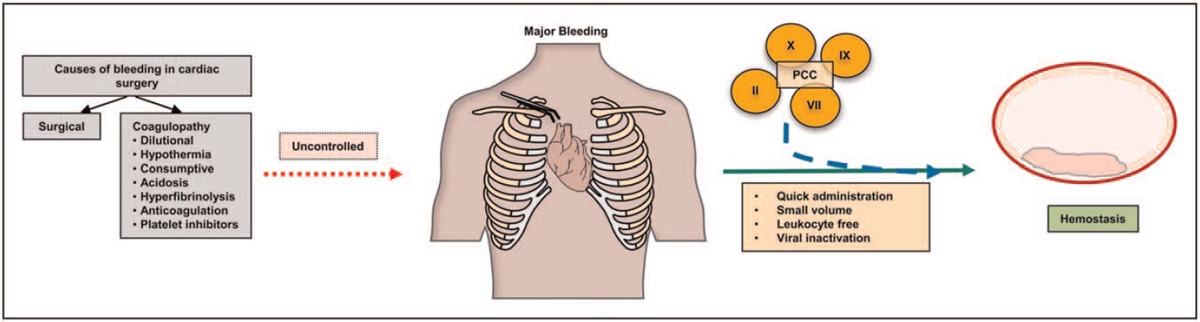
Was reviewing some literature for control of coagulopathy in cardiac surgery. I was wondering if you or your centers routinely use PCC now instead of FFP. If so, what doses do you normally use? We don't have ROTEM or TEG here but our department is considering moving to PCCs as first line now.
Here is a recent review:
 journals.lww.com
journals.lww.com
Was reviewing some literature for control of coagulopathy in cardiac surgery. I was wondering if you or your centers routinely use PCC now instead of FFP. If so, what doses do you normally use? We don't have ROTEM or TEG here but our department is considering moving to PCCs as first line now.
Here is a recent review:
Prothrombin complex concentrates in cardiac surgery: where... : Current Opinion in Anesthesiology
These findings have led to off-label uses of prothrombin complex concentrates (PCCs) in cardiac surgery. The purpose of this review is to compare and contrast the use of FFP and PCC, review the components, limitations and risks of different types of PCCs, and discuss the latest evidence for the...
journals.lww.com