You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Cleviprex
Started by BLADEMDA


I'm starting to use a lot of this stuff and wanted opinions on any "negatives" you have seen so far. Fast onset (1 minute) and Fast offset (2-3 minutes) with a terminal elimination of 15 minutes. This seems like a great drug for anesthesia.
Anyone have experience with IV bolus doses? I'm talking about giving a quick 0.25-0.5 mg mg IV push of Cleviprex to get the BP down then start the infusion. Or, maybe just 0.25-0.5 mg IV x 1 for wake-up or post intubation.
Anyone dilute this stuff up with NS and place in a syringe? Since this is a LIPID based drug I'm not sure how long it is stable when diluted with NS. My guess is 1-2 hours at most.
Dilution with NS would allow me to titrate the drug better as an IV bolus dose.
Comments?
FYI, this stuff is very cost-effective and I strongly urge you to look at this drug vs NTP in terms of cost.
Anyone have experience with IV bolus doses? I'm talking about giving a quick 0.25-0.5 mg mg IV push of Cleviprex to get the BP down then start the infusion. Or, maybe just 0.25-0.5 mg IV x 1 for wake-up or post intubation.
Anyone dilute this stuff up with NS and place in a syringe? Since this is a LIPID based drug I'm not sure how long it is stable when diluted with NS. My guess is 1-2 hours at most.
Dilution with NS would allow me to titrate the drug better as an IV bolus dose.
Comments?
FYI, this stuff is very cost-effective and I strongly urge you to look at this drug vs NTP in terms of cost.

Drugs. 2014 Oct;74(16):1947-60. doi: 10.1007/s40265-014-0313-6.
Clevidipine: a review of its use for managing blood pressure in perioperative and intensive care settings.
Keating GM1.
Author information
Abstract
The ultrashort-acting dihydropyridine calcium channel antagonist clevidipine (Cleviprex(®)) has a rapid onset and offset of effect and reduces blood pressure (BP) by decreasing arteriolar resistance without affecting venous capacitance vessels. This article reviews the clinical efficacy and tolerability of intravenous clevidipine when used to manage BP in perioperative and intensive care settings, as well as summarizing its pharmacological properties. Intravenous clevidipine effectively treated preoperative and postoperative hypertension in patients undergoing cardiac surgery, according to the results of the randomized, multicentre, double-blind, phase III ESCAPE-1 and ESCAPE-2 trials. The randomized, open-label, multicentre, phase III ECLIPSE trials indicated that in terms of keeping systolic BP within the target range, clevidipine was more effective than nitroglycerin or sodium nitroprusside perioperatively and had similar efficacy to nicardipine postoperatively in cardiac surgery patients. In small, double-blind trials in patients undergoing coronary artery bypass graft surgery, perioperative clevidipine was noninferior to nitroglycerin, and postoperative clevidipine had similar efficacy to sodium nitroprusside. Noncomparative studies demonstrated that clevidipine provided rapid BP control in patients with acute neurological injuries (including intracerebral haemorrhage, subarachnoid haemorrhage and acute ischaemic stroke), and was not associated with 'overshoot' in the vast majority of patients. Intravenous clevidipine was generally well tolerated and was usually associated with no reflex tachycardia or only very modest increases in heart rate. In conclusion, intravenous clevidipine is a valuable agent for the management of BP in perioperative and intensive care settings.
Clevidipine: a review of its use for managing blood pressure in perioperative and intensive care settings.
Keating GM1.
Author information
Abstract
The ultrashort-acting dihydropyridine calcium channel antagonist clevidipine (Cleviprex(®)) has a rapid onset and offset of effect and reduces blood pressure (BP) by decreasing arteriolar resistance without affecting venous capacitance vessels. This article reviews the clinical efficacy and tolerability of intravenous clevidipine when used to manage BP in perioperative and intensive care settings, as well as summarizing its pharmacological properties. Intravenous clevidipine effectively treated preoperative and postoperative hypertension in patients undergoing cardiac surgery, according to the results of the randomized, multicentre, double-blind, phase III ESCAPE-1 and ESCAPE-2 trials. The randomized, open-label, multicentre, phase III ECLIPSE trials indicated that in terms of keeping systolic BP within the target range, clevidipine was more effective than nitroglycerin or sodium nitroprusside perioperatively and had similar efficacy to nicardipine postoperatively in cardiac surgery patients. In small, double-blind trials in patients undergoing coronary artery bypass graft surgery, perioperative clevidipine was noninferior to nitroglycerin, and postoperative clevidipine had similar efficacy to sodium nitroprusside. Noncomparative studies demonstrated that clevidipine provided rapid BP control in patients with acute neurological injuries (including intracerebral haemorrhage, subarachnoid haemorrhage and acute ischaemic stroke), and was not associated with 'overshoot' in the vast majority of patients. Intravenous clevidipine was generally well tolerated and was usually associated with no reflex tachycardia or only very modest increases in heart rate. In conclusion, intravenous clevidipine is a valuable agent for the management of BP in perioperative and intensive care settings.
Clevidipine is rapidly distributed and metabolized resulting in a very short half life. The arterial blood concentration of clevidipine declines in a multi-phasic pattern following termination of the infusion. The initial phase half-life is approximately 1 minute, and accounts for 85-90% of clevidipine elimination. The terminal half-life is approximately 15 minutes.

Haven't used it since med school so I can't say much about it. We still buy Cardene bags at our institution although we do have some 2.5mg/ml vials of what looks like generic nicardipine lying around. My understanding is that even the generic nicardipine IV is still expensive (can anyone confirm/deny?) to the point where cleviprex costs the same, and as such it's a superior drug...
That being said, I'd be surprised if I could tell a speed difference between pushing cardene 100mcg, ntg 50mcg, or whatever bolus of cleviprex
That being said, I'd be surprised if I could tell a speed difference between pushing cardene 100mcg, ntg 50mcg, or whatever bolus of cleviprex
Recently got it added to formulary at our place and I think it's getting good acceptance. It seems like a decent alternative to nicardipine. The lipid formulation of it does prevent prolonged usage in the ICU.
Biggest down side of clevprex: it looks like propofol. Half a cc will drop your map 20 points. An accidental full syringe mistaken as propofol will kill you.
Advertisement - Members don't see this ad
D
deleted59964
Biggest down side of clevprex: it looks like propofol. Half a cc will drop your map 20 points. An accidental full syringe mistaken as propofol will kill you.
yikes - that is a major risk ... why the hell can't they color it!
I was taught to put a mL of methylene blue in bags of succinylcholine used for infusions.yikes - that is a major risk ... why the hell can't they color it!
As I recall methylene blue is kind of expensive though.
You got stock in this drug, Blade?
There are no drawbacks.
Best antipertensive out there. Hands down.
Use it in the heart room just about every time.
Nitro and Nitroprusside I rarely use now.
Best antipertensive out there. Hands down.
Use it in the heart room just about every time.
Nitro and Nitroprusside I rarely use now.
NTG works a tad bit faster, but you can dial in cleviprex with ease... it's almost like cheating.
I'm starting to use a lot of this stuff and wanted opinions on any "negatives" you have seen so far. Fast onset (1 minute) and Fast offset (2-3 minutes) with a terminal elimination of 15 minutes. This seems like a great drug for anesthesia.
What advantages does it have vs nitroprusside?
What advantages does it have vs nitroprusside?
NTP costs TEN TIMES more than Cleviprex at my hospital. We can buy 10 bottles of Cleviprex for the price of one vial of NTP.
Valeant has been purchasing drugs from other pharmas (and smaller pharmas too) and jacking up the drug price on the very day the deal is signed. Valeant Nitroprusside (which is used to lower blood pressure in emergencies) and Isoproterenol (used to speed up the heart rate and raise blood pressure in emergencies) from AstraZeneca on February 10. Nitroprusside price went up by factor of over 5 and Isoproterenol by a factor of over 2 on February 10. That very day!
More pharmaceutical companies are buying drugs that they see as undervalued, then raising the prices. It is one of a number of industry tactics, along with companies regularly upping the prices of their own older medicines and launching new treatments at once unheard of sums, driving up the cost of drugs.
More pharmaceutical companies are buying drugs that they see as undervalued, then raising the prices. It is one of a number of industry tactics, along with companies regularly upping the prices of their own older medicines and launching new treatments at once unheard of sums, driving up the cost of drugs.

BETHESDA, MD 01 Feb 2016—When the staff at Baystate Health in Massachusetts observed an alarming series of price increases for the vasodilator drug nitroprusside last year, the integrated health system took a strong step in response.
"Over a period of time during 2015, we just basically booted nitroprusside out of the building," said Gary Kerr, chief pharmacy officer for the health system.
Nitroprusside and an inotropic drug, isoproterenol, sold by Valeant Pharmaceuticals International, Inc., were among the medications discussed during a December 9 Senate Special Committee on Aging hearing that examined sudden price spikes affecting off-patent drug products.
Valeant's website states that the company markets more than 200 prescription drug products. The company has made headlines and angered legislators by purchasing the rights to older drugs and then dramatically increasing their prices.
"We're very acutely aware of drug prices," Kerr said. "Part of our modus operandi here has always been to manage our drug utilization, our drug selection, and our budgets as thoughtfully as we can."
He said the "dramatic and sudden" increase in the price of nitroprusside was debated in a series of pharmacy and therapeutics committee meetings last year, with active input from three surgical departments and the emergency department physicians.
Kerr said the group compared normalized treatment costs for nitroprusside and two alternative drugs—clevidipine and nicardipine—and ultimately decided to drop nitroprusside from the formulary.
The new treatment cost for nitroprusside would be 8 to about 60 times the cost for the alternative drugs' vials or premixed injection, according to Kerr's figures.
Kerr said the health system's physicians supported the formulary decision even though it meant changes to patient care.
"There are some nuances with the drugs and their indications, but the docs are very, very cooperative with us. They know that the . . . drug formulary is a critical management tool for us," Kerr said.
Joel Melroy, manager of adult inpatient pharmacy services for Medical University of South Carolina (MUSC) Hospital Authority, similarly emphasized pharmacy's role in managing drug costs.
"We, as pharmacists, are in the business of ensuring that our patients have the best therapy and the most cost-effective therapy to the patient, to the hospital, and to the payer," Melroy said.
Melroy said last year's increases in the price of nitroprusside, a relatively low-use drug, weren't a major issue for the health system. But the increased cost of isoproterenol was a problem.
Melroy said the pharmacy team analyzed where and how the drug was being used in the hospital and concluded that stocking smaller vials of the drug would blunt the price increase.
"We've tried to soften the impact as much as we can by doing what we can—which is actually very little—to decrease the cost that the hospital and the health system is actually incurring," he said.
Jerome Wohleb, director of pharmacy services at Bryan Medical Center in Lincoln, Nebraska, said the pharmacy previously prepared i.v. bags with isoproterenol for use as needed in the cardiology service and the intensive care unit.
"Now, we don't mix it up until [it's time] to hang it, which means a physician says, 'I've got to have it,'" Wohleb said.
To similarly minimize the waste of nitroprusside, he said, "We've tried to reduce the sizes of our mixed products and watched how we are administering it."
Wohleb emphasized that the problem of price increases affects "substantially more" than just the two Valeant drugs.
He said the price for the 20 most costly drugs purchased by the hospital in the past 18 months has increased by 11%, on average, or about $2 million. For workhorse drugs that are widely used throughout the hospital, such as analgesics, anesthesia drugs, and surgical drugs, the cost increases over 18 months have ranged from 126% to 5000%.
Wohleb said his medical center "really is counting on the pharmacy to be a solution" to the problem of high drug costs.
"What we've done here to counter this change is to really beef up our clinical services, and try to work collaboratively with physicians, and target some of our expensive drugs so that we can appropriately use drugs that are needed," Wohleb said. He said an active therapeutic interchange program is a big part of that effort.
Jason Mills, pharmacy supply chain manager for MUSC Hospital Authority, noted that there are drawbacks to changing long-established medication therapy for reasons other than clinical benefit.
"The drugs in the Valeant catalog are staples. They're old drugs. They've got the proof that the evidence-based practice is there. It's really hard to drive practice change when you've got decades of proof that this agent is effective," Mills said.
Such changes also affect the implementation of order sets and various parts of the medication-use process.
"We heavily use barcode scanning on different phases of our distribution process," Melroy said. That means, he said, that whenever MUSC's pharmacy distributes a drug product that has a different National Drug Code number than a previously distributed product, "there is a lot behind the scenes that has to happen" to ensure the change is recognized by the order sets that specify the drug.
Mills said the same issues arise when the hospital makes purchasing changes in response to drug shortages. But he said there's often less mystery associated with shortages than with price increases.
"With a shortage, you're kind of dealing with a fixed timeline. Typically, you reach out to the manufacturers, and they give you an estimate as to when the product in question is going to get back into the supply chain or if it's been discontinued outright. So you have a little more clarity," Mills said.
Kerr said that in the past, Baystate took little notice of the weekly reports on drug price changes from the health system's wholesaler.
"We're paying attention right now," Kerr said. "You've got to have an infrastructure, and you've got to have people committed to this. . . . This is something you've got to manage every week, if not every day."
A statement posted on Valeant's website in response to the December 9 Senate hearing explains that because most hospitals use small amounts of isoproterenol and nitroprusside, the price increase "has had a limited impact on the average hospital's cost." The company also stated that it is working with "the small number of hospitals who use a large volume of the drugs" to provide "significant volume discounts."
Erin R. Fox, director of the drug information service for University of Utah Health Care, testified during the Senate hearing that she had called Valeant to negotiate price concessions for isoproterenol and nitroprusside.
"Each time I called, I was referred back to my wholesaler for the purchase price," she said. "Each time, the answer was, 'Talk to your distributor.'"
- See more at: http://www.ashp.org/menu/News/PharmacyNews/NewsArticle.aspx?id=4301#sthash.rRUXrqZh.dpuf
"Over a period of time during 2015, we just basically booted nitroprusside out of the building," said Gary Kerr, chief pharmacy officer for the health system.
Nitroprusside and an inotropic drug, isoproterenol, sold by Valeant Pharmaceuticals International, Inc., were among the medications discussed during a December 9 Senate Special Committee on Aging hearing that examined sudden price spikes affecting off-patent drug products.
Valeant's website states that the company markets more than 200 prescription drug products. The company has made headlines and angered legislators by purchasing the rights to older drugs and then dramatically increasing their prices.
"We're very acutely aware of drug prices," Kerr said. "Part of our modus operandi here has always been to manage our drug utilization, our drug selection, and our budgets as thoughtfully as we can."
He said the "dramatic and sudden" increase in the price of nitroprusside was debated in a series of pharmacy and therapeutics committee meetings last year, with active input from three surgical departments and the emergency department physicians.
Kerr said the group compared normalized treatment costs for nitroprusside and two alternative drugs—clevidipine and nicardipine—and ultimately decided to drop nitroprusside from the formulary.
The new treatment cost for nitroprusside would be 8 to about 60 times the cost for the alternative drugs' vials or premixed injection, according to Kerr's figures.
Kerr said the health system's physicians supported the formulary decision even though it meant changes to patient care.
"There are some nuances with the drugs and their indications, but the docs are very, very cooperative with us. They know that the . . . drug formulary is a critical management tool for us," Kerr said.
Joel Melroy, manager of adult inpatient pharmacy services for Medical University of South Carolina (MUSC) Hospital Authority, similarly emphasized pharmacy's role in managing drug costs.
"We, as pharmacists, are in the business of ensuring that our patients have the best therapy and the most cost-effective therapy to the patient, to the hospital, and to the payer," Melroy said.
Melroy said last year's increases in the price of nitroprusside, a relatively low-use drug, weren't a major issue for the health system. But the increased cost of isoproterenol was a problem.
Melroy said the pharmacy team analyzed where and how the drug was being used in the hospital and concluded that stocking smaller vials of the drug would blunt the price increase.
"We've tried to soften the impact as much as we can by doing what we can—which is actually very little—to decrease the cost that the hospital and the health system is actually incurring," he said.
Jerome Wohleb, director of pharmacy services at Bryan Medical Center in Lincoln, Nebraska, said the pharmacy previously prepared i.v. bags with isoproterenol for use as needed in the cardiology service and the intensive care unit.
"Now, we don't mix it up until [it's time] to hang it, which means a physician says, 'I've got to have it,'" Wohleb said.
To similarly minimize the waste of nitroprusside, he said, "We've tried to reduce the sizes of our mixed products and watched how we are administering it."
Wohleb emphasized that the problem of price increases affects "substantially more" than just the two Valeant drugs.
He said the price for the 20 most costly drugs purchased by the hospital in the past 18 months has increased by 11%, on average, or about $2 million. For workhorse drugs that are widely used throughout the hospital, such as analgesics, anesthesia drugs, and surgical drugs, the cost increases over 18 months have ranged from 126% to 5000%.
Wohleb said his medical center "really is counting on the pharmacy to be a solution" to the problem of high drug costs.
"What we've done here to counter this change is to really beef up our clinical services, and try to work collaboratively with physicians, and target some of our expensive drugs so that we can appropriately use drugs that are needed," Wohleb said. He said an active therapeutic interchange program is a big part of that effort.
Jason Mills, pharmacy supply chain manager for MUSC Hospital Authority, noted that there are drawbacks to changing long-established medication therapy for reasons other than clinical benefit.
"The drugs in the Valeant catalog are staples. They're old drugs. They've got the proof that the evidence-based practice is there. It's really hard to drive practice change when you've got decades of proof that this agent is effective," Mills said.
Such changes also affect the implementation of order sets and various parts of the medication-use process.
"We heavily use barcode scanning on different phases of our distribution process," Melroy said. That means, he said, that whenever MUSC's pharmacy distributes a drug product that has a different National Drug Code number than a previously distributed product, "there is a lot behind the scenes that has to happen" to ensure the change is recognized by the order sets that specify the drug.
Mills said the same issues arise when the hospital makes purchasing changes in response to drug shortages. But he said there's often less mystery associated with shortages than with price increases.
"With a shortage, you're kind of dealing with a fixed timeline. Typically, you reach out to the manufacturers, and they give you an estimate as to when the product in question is going to get back into the supply chain or if it's been discontinued outright. So you have a little more clarity," Mills said.
Kerr said that in the past, Baystate took little notice of the weekly reports on drug price changes from the health system's wholesaler.
"We're paying attention right now," Kerr said. "You've got to have an infrastructure, and you've got to have people committed to this. . . . This is something you've got to manage every week, if not every day."
A statement posted on Valeant's website in response to the December 9 Senate hearing explains that because most hospitals use small amounts of isoproterenol and nitroprusside, the price increase "has had a limited impact on the average hospital's cost." The company also stated that it is working with "the small number of hospitals who use a large volume of the drugs" to provide "significant volume discounts."
Erin R. Fox, director of the drug information service for University of Utah Health Care, testified during the Senate hearing that she had called Valeant to negotiate price concessions for isoproterenol and nitroprusside.
"Each time I called, I was referred back to my wholesaler for the purchase price," she said. "Each time, the answer was, 'Talk to your distributor.'"
- See more at: http://www.ashp.org/menu/News/PharmacyNews/NewsArticle.aspx?id=4301#sthash.rRUXrqZh.dpuf
Advertisement - Members don't see this ad
D
deleted162650
Yup. Not long ago I had our OR pharmacist come into my room after I ordered an SNP gtt practically begging me to use Nicardipine next time since its now an order of magnitude cheaper than SNP. Sad but true.
Just got it added to our OR stock. Thanks.
Use it in the heart room just about every time.
Every case? What are you using it for? To bring bp down for cannulation?
clevidipine is an awesome drug. it's an calcium channel blocker and a pure afterload reduction agent. i don't use it as a bolus, only as a drip. it's a great drug when you expect extreme hemodynamic fluctuation. I mainly use it for open AAA. i can imagine using it for pheo resection but obviously pheo is not a common surgery done in the community. you must educate the hell out of nurses in the ICU and recovery area as some people might think it is propofol. we have it as non-formulary but hopefully it will become formulary soon.
I mainly use it for open AAA.
How many of those are you doing? Those have gone the way of the Dodo at my institution.
Been using a while, not bolusing it. Great for coming off bypass, real stable quick titrations. Usually double the does every couple minutes and then a few small titrations between the new and the last dose. Interestingly had a couple patients "fail" cleviprex but do well with cardene. I compare cleviprex to remi and cardene to precedex in terms of onset of action as ease of titration in the OR.
IMHO any person who confuses Cleviprex with propofol practices very sloppy anesthesia, especially considering EVERY OTHER DRUG is the color of WATER. Never heard anyone complain that there were too many drugs that looked like water!
IMHO any person who confuses Cleviprex with propofol practices very sloppy anesthesia, especially considering EVERY OTHER DRUG is the color of WATER. Never heard anyone complain that there were too many drugs that looked like water!
Been using a while, not bolusing it. Great for coming off bypass, real stable quick titrations.
Am I missing something? I'm usually reaching for constrictors when coming off, not dilators. You come off with a dilator? Why would that be?
We have had this drug for a while now but I hardly ever seen an scenario where it would be needed.
How many of those are you doing? Those have gone the way of the Dodo at my institution.
being a quartenary/tertiary center, we do quite a few of open repairs. these are not run of the mill EVARs, but more like enormous AAA or TAA-AAA which often gets repaired as two-staged surgeries. it's definitely no dodo here, more of a rare species.
Every case? What are you using it for? To bring bp down for cannulation?
Nah... I usually give a small bump of prop for that if I need it. I always leave the nurses in the CTICU with an upper and a downer gtt inline and ready to go. It is part of my routine.
Always epi and always cleviprex. Sometimes I'll add to that vaso and/or norepi depending on the case. I've stopped using dopamine, NTG, and nitroprusside for the most part. I may use NTG or NTG/EPI with a loading dose of milrinone for severe pulm. htn/RV failure.
That being said, for my AVRs, MVRs, aortic roots, double valves, DHCAs, even CABs I keep my BP in a pretty tight range and unless there is a reason to keep the BP higher, I dial it in around 95-110 systolic. Clevidipine makes attaining this goal easy especially as you washout your iso and are heading up to the unit with a little dex.
The gtt volume I need to attain a certain BP in a tough hypertensive patient is miniscule compared to NTG. I have seen NTG and Nitroprusside fail when Cleviprex just nails it.
You can bolus Cleviprex. Take a cc or two and dilute it into 10ccs. Bolus it one cc at a time. It works very well, but not better than prop IMO--- clevidipine lingers around a bit longer, but will control most any hypertensive patient when other methods fail.
Love that stuff... it's like cardiac anesthesia crack for me.
I see cleviprex as a titration drug as it's primary use. Don't like to bolus it unless I have to.
Advertisement - Members don't see this ad
IMHO any person who confuses Cleviprex with propofol practices very sloppy anesthesia, especially considering EVERY OTHER DRUG is the color of WATER. Never heard anyone complain that there were too many drugs that looked like water!
Precisely the problem. For many years there has been only 1 white drug. Now, once everyone knows what a white syringe means, they introduce a second one which looks exactly the same. It's a setup for medical mistakes.
OTOH, why not color-code all families of drugs from now on?
Induction agents: white
Analgesics: blue
Anxiolytics: yellow
Paralytics: red
Antibiotics: green
etc
etc
etc
Sounds reasonable.Nah... I usually give a small bump of prop for that if I need it. I always leave the nurses in the CTICU with an upper and a downer gtt inline and ready to go. It is part of my routine.
Always epi and always cleviprex. Sometimes I'll add to that vaso and/or norepi depending on the case. I've stopped using dopamine, NTG, and nitroprusside for the most part. I may use NTG or NTG/EPI with a loading dose of milrinone for severe pulm. htn/RV failure.
That being said, for my AVRs, MVRs, aortic roots, double valves, DHCAs, even CABs I keep my BP in a pretty tight range and unless there is a reason to keep the BP higher, I dial it in around 95-110 systolic. Clevidipine makes attaining this goal easy especially as you washout your iso and are heading up to the unit with a little dex.
The gtt volume I need to attain a certain BP in a tough hypertensive patient is miniscule compared to NTG. I have seen NTG and Nitroprusside fail when Cleviprex just nails it.
You can bolus Cleviprex. Take a cc or two and dilute it into 10ccs. Bolus it one cc at a time. It works very well, but not better than prop IMO--- clevidipine lingers around a bit longer, but will control most any hypertensive patient when other methods fail.
Love that stuff... it's like cardiac anesthesia crack for me.
I'm not ready to make the jump just yet.
A quick Google search says that the drug should be discarded every 4 hours , and it is associated with increased risk of a fib.
http://www.medscape.com/viewarticle/720024_7
Last edited:
I believe the package insert says 12 hours. I'll check today.
The afib is a weak association, likely due to clevidipine being used more often in valve cases- Afib was still within the norm for cardiac surgical patients however.
Give it a go, I think you'll like it. 👍
The afib is a weak association, likely due to clevidipine being used more often in valve cases- Afib was still within the norm for cardiac surgical patients however.
Give it a go, I think you'll like it. 👍
Precisely the problem. For many years there has been only 1 white drug. Now, once everyone knows what a white syringe means, they introduce a second one which looks exactly the same. It's a setup for medical mistakes.
OTOH, why not color-code all families of drugs from now on?
Induction agents: white
Analgesics: blue
Anxiolytics: yellow
Paralytics: red
Antibiotics: green
etc
etc
etc
Induction agents have yellow stickers.
Anxiolytics have orange ones.
Agree with Seinfeld. You're being sloppy if you can't correctly label your drugs and routinely get them confused. That's anesthesia 101.
In the case of a syringe of cleviprex, I have a big 'ol generic red sticker on it. Impossible to confuse with anything else.
I have seen some other stuff saying 12 hours.I believe the package insert says 12 hours. I'll check today.
The afib is a weak association, likely due to clevidipine being used more often in valve cases- Afib was still within the norm for cardiac surgical patients however.
Give it a go, I think you'll like it. 👍
On the a fib I'm not so clear. They halted a study for this, but then they said it was no different than other drugs.
There are also hints of higher acute kidney injury.
I would like to see a non company sponsored trial for this.
Arch Guillotti
Senior Member
Staff member
Administrator
Volunteer Staff
Lifetime Donor
20+ Year Member
Precisely the problem. For many years there has been only 1 white drug. Now, once everyone knows what a white syringe means, they introduce a second one which looks exactly the same. It's a setup for medical mistakes.
OTOH, why not color-code all families of drugs from now on?
Induction agents: white
Analgesics: blue
Anxiolytics: yellow
Paralytics: red
Antibiotics: green
etc
etc
etc
It isn't a setup for mistakes anymore than it is now. Mistakes happen no matter what when people are in a rush or don't pay attention.
Drugs already are color coded by label to some degree.


Induction agents have yellow stickers.
Anxiolytics have orange ones.
Agree with Seinfeld. You're being sloppy if you can't correctly label your drugs and routinely get them confused. That's anesthesia 101.
In the case of a syringe of cleviprex, I have a big 'ol generic red sticker on it. Impossible to confuse with anything else.
I didn't mean stickers. I meant the color of the fluid itself.
Am I missing something? I'm usually reaching for constrictors when coming off, not dilators. You come off with a dilator? Why would that be?
We have had this drug for a while now but I hardly ever seen an scenario where it would be needed.
For our Aortic work (AVRs, Bentals, Ascending, dissections repairs, transaortic TAVRs) we do use anti-HTN about 30% of the time. Surgeons routinely want SBP 90-100.
Advertisement - Members don't see this ad
Last I checked (last winter) at our place it was about $4/bottle, but was on a national shortage. Lymphazurin blue was far more expensive, like $400/vial. But that price could have easily changed.I was taught to put a mL of methylene blue in bags of succinylcholine used for infusions.
As I recall methylene blue is kind of expensive though.
D
deleted162650
We've been out of methylene blue for a while too. Even indigo carmine is a pain to get. Never seen lymphazurin used for anything besides SNBs
Me either. I got the honor of having to present an M&M while off-service and I did some digging into cost. Holy crap, lymphazurin blue is expensive! And frankly, not that much better than methylene blue when used for peritumor injection at localizing the SLN.We've been out of methylene blue for a while too. Even indigo carmine is a pain to get. Never seen lymphazurin used for anything besides SNBs
I like Cleviprex. We use it on our CEA's and our very rare open AAA. Very titratable.
I rarely need to use something to get the BP down in carotids. Usually, it's neo to get it up enough.
I rarely need to use something to get the BP down in carotids. Usually, it's neo to get it up enough.
Seriously? Half our carotids are old brittle hypertensives who come in day of surgery SBP 160++. Usually need cardene around incision and emergence/PACU, neo for induction and middle part of the procedure.
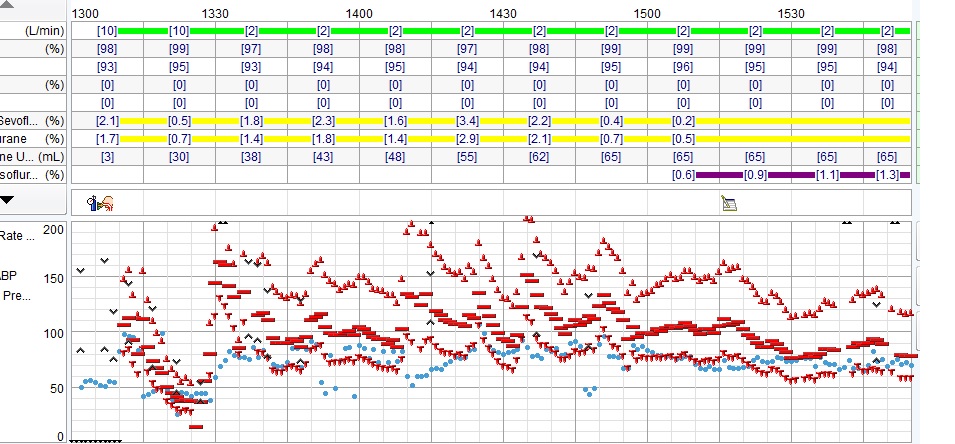
OCD infusion titration and bolusing of cardene and neo is how I get my CEAs to look like this
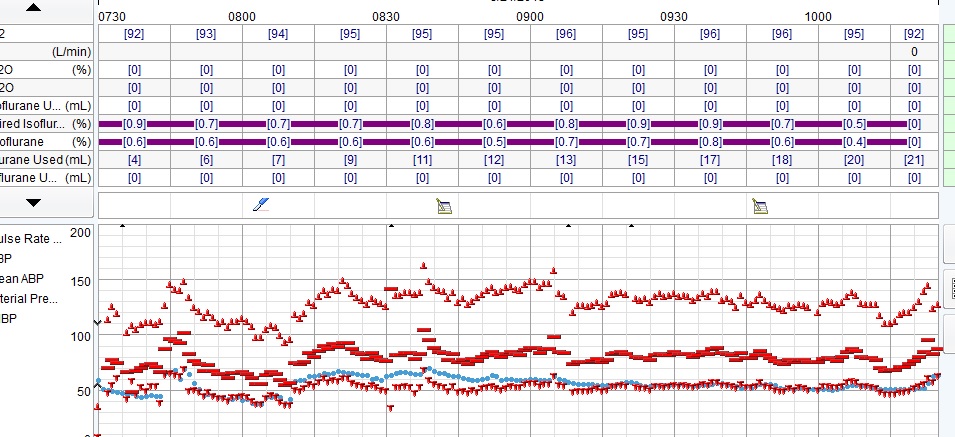
and not this (CRNA)
Last edited:
Only half of your carotids are old brittle hypertensives?Seriously? Half our carotids are old brittle hypertensives who come in day of surgery SBP 160++. Usually need cardene around incision and emergence/PACU, neo for induction and middle part of the procedure.
And what's your target MAP during the repair part of the case?
Yeah... seems a bit odd to load up a vasodilator for a CEA case where you actually want to keep them w/in 20% of their baseline and then go up on that when cross clamped.
I honestly can't remember the last CEA I had a vasoodilator infusion going.
But people do things differently.
I honestly can't remember the last CEA I had a vasoodilator infusion going.
But people do things differently.
That CRNA record is horrid btw. If I'm reading that right... I see a systolic of 55 followed by one of 200.
Looks like that scenario played out a couple of times during the case. 😵
Looks like that scenario played out a couple of times during the case. 😵
Neat thing about electronic records is they keep people honest ...That CRNA record is horrid btw. If I'm reading that right... I see a systolic of 55 followed by one of 200.
Looks like that scenario played out a couple of times during the case. 😵
Advertisement - Members don't see this ad