
- Joined
- Aug 31, 2008
- Messages
- 306
- Reaction score
- 20
The argument below is an argument that consciousness ceases at death. It isn't about clinical neurology per se, but it uses a lot of examples from clinical neurology. I was wondering if any of you had any opinions about my argument.
enjoy
")
--------
Consciousness is the feature of self-awareness, the ability to perceive sensation, and the ability to think. It is often characterized as having an emotional state and internal volition.
My central point is that the mind is a direct manifestation of the physical brain.
That is, all of sensation, emotion, perception, thought, memory, personality, self awareness, and volition is a result of the properties of the gelatinous organ between your ears.
Allow me to build my case by providing a large number of examples from clinical neurology. This may seem somewhat tedious, but I am trying to develop the idea that the mind is not a black box. It is quite well understood, and there is no longer any need to guess at its functions. I am attempting to give specific detailed examples. My format is 1) sensory modality, 2) anatomy (where it is located in the brain), 3) pathology (how it is destroyed in disease states)
Sensation:
vibration sensation of the skin:
vibration is sensed by small organs called pacinian corpuscles in the skin. Information is carried through large myelinated fibers to the dorsal column, the medial lemniscus, the ventral posterolateral nucleus of the thalamus, and ultimately to the contralateral primary somatosensory cortex.
Destruction of any of these areas leads to a loss of vibration sensation.
examples:
1) The dorsal column in syphilis
2) The somatosensory cortex in middle cerebral artery stroke
vision:
The electromagnetic stimulation of light is translated into an electrochemical signal in the rods and cones in the retina which is ultimately transferred to bipolar cells and then ganglion cells whose axons converge to form the optic nerve, the optic chiasm, the optic tract...and ultimately synapse in the primary visual cortex (Brodmann's area 17) which interacts with association areas in complex ways.
Damage to various components of the visual system can cause different consequences
examples:
1) macular degeneration can cause distortion of visual images (though accumulation of drusen in the retina)
2) Compresion of the optic chiasm by a pituitary adenoma (a tumor of the pituitary gland) can cause tunnel vision (bitemporal hemianopia).
3) A stroke in the posterior cerebral artery can cause loss of vision to one side (homonymous hemianopia) with sparing of central vision (macular sparing)
4) brain tumors in the occipitotemporal area can (rarely) cause the inability to recognize complex objects or even specifically the ability to recognize faces (aprosopagnosia). This is related to the inability to process and interpret complex visual data.
This all likely comes off as being esoteric and turgid. That is not my intention. My intention is to emphasize how well understood neurology is. Of course...you would never question me on this. You know that vibration sensation and vision are organic phenomena which are purely the result of the physical brain. They do not require supernatural explanations. They do not require a soul or a spirit to work. The argument which I am making is that these aspects of consciousness are perhaps more well understood but no less supernatural than other aspects of consciousness. Allow me to continue.
memory:
Memory involves the linking of various areas of the brain and changing of the properties of synaptic connections
it is mediated to a large extent by the papez circuit below:
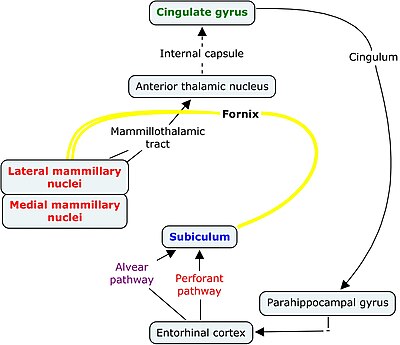
complex information from all aspects of the nervous system enter the subiculum of the hippocampus from the parahippocampal gyrus and entorhinal cortex. The hippocampus itself is responsible for the formation of the new circuits. This is believed to occur through upregulation of glutamate receptors (glutamate is an excitatory neurotransmitter) so that a new or modified ability of one neuron to act on another is created. This information is then relayed to the cingulate gyrus which is responsible for much of the emotional significance or emotional content of memory.
Note: Different forms of memory are believed to be formed in different ways. For example, the cerebellum plays a large role in memory of fine procedural coordination (motor memory)
Memory can be altered in various ways clinically.
1) Simple amnestic seizure. In very rare cases, a seizure in the hipocampus on the dominant side can cause amnesia for the time period while the seizure is occurring with no other symptoms.
2) Transient global amnesia. this a rare syndrome where a patient loses the ability to form new memories for several hours. The patient often repeats questions over and over and then recovers completely. Some of these cases are believed to be due to poor venous drainage from the hippocampus.
3) korsakoff's syndrome-this is caused by vitamin B1 (thiamine) deficiency often seen in alcoholics which leads to bilateral hemorrhage and destruction of the mamillary bodies (see diagram above). The result is a permanent inability to form new memories (similar to the protagonist in the movie Memento)
4) In the past, it was common to perform a temporal lobectomy (removal of the temporal lobe) in patients with seizure disorders to control seizures. This would very commonly lead to severe defects in spatial memory.
5) In Alzheimers dementia, amyloid plaques accumulate in cells, leading to neuronal death, particularly in the temporal and frontal lobes. This initially causes short term memory difficulties and ultimately profound amnesia.
emotion:
Surely, emotion is a complex phenomenon. Much of emotion is believed to be related to the interaction of the limbic system. Here are some pieces of the puzzle:
The anterior nucleus of the thalamus receives the mamillothalamic tract and projects to the cingulate gyrus, linking memory with the main gyrus which regulates emotion.
The amygdala (which lies adjacent to the parahippocampal gyrus) causes fear and a sort of "fight or flight" response when stimulated (in addition to the anterior nucleus of the hypothalamus).
The nucleus accumbens is located in the basal ganglia and contains many dopaminergic neurons (neurons which use dopamine as a neurotransmitter). It has a known involvement in pleasure, reward, addiction, and the placebo effect.
Clinical correlates
1) The herpes virus can rarely cause an encephalitis (brain inflammation) syndrome which can cause destruction of the amygdala. This can lead to what is known as "kluver bucy syndrome." Patients with this syndrome are extremely placid. They lose their normal responses of fear and anger to stimuli, and they exhibit unusual improper sexual behavior (such as indiscriminately trying to have sex with inanimate objects)
2) abnormalities in the serotonin producing neurons in the raphe nuclei and norepinephrine producing neurons in the locus ceruleus are believed to be related to symptoms of depression and anxiety, and various drug treatments target these receptors.
3) Pleasure causing drugs such as heroin indirectly cause increased dopaminergic release in the nucleus accumbens which causes the sensation of incredible euphoria. Prolonged stimulation can cause downregulation of the dopamine receptors which can lead to physical dependence, anhedonia during withdrawal, and drug addiction
Personality:
Some aspects of personality are related closely with other systems (see kluver bucy syndrome). However, personality is dependent not only on deep seated nuclei in the brain (the amygdala, the cingulate gyrus, etc.) but also the more rostral structures such as the prefrontal cortex. These areas are also related to "higher" thought processes such as judgment, planning, morality, and logic. I'll simply discuss some cases.
1) There is a very famous case of a man named Phineas P. Gage who worked as a railroad construction foreman during the 19th century. He was injured by a large iron rod which was driven through the front of his skull, destroying much of his frontal lobe. After the event, he had an excellent recovery. However, he was noted by his peers to have various personality changes. He was childish, profane, and disinhibited on some accounts.
2) The procedure known as frontal lobotomy (destruction of the frontal lobe) was performed in a large number of patients for various psychiatric problems in the early 20th century. Destruction of the right frontal lobe would at times induce mania in depressed individuals. Destruction of the left frontal lobe would at times cause apathy or resolution of mania in the angry or manic patient respectively.
3) There are cases of right frontal lobe strokes and tumors which cause mania. Left frontal lobe stroke is associated with severe depression.
Self awareness:
Various experiments have determined that alertness, ability to process information, and reaction to stimuli is dependent on activity of the cortex (the surface) of the brain. There are various intermediate states of consciousness which occur during sleep or occur on a subconscious level, but all of these require activation of the cortex. Patients who are brain dead, for instance, do not exhibit sleep cycle changes associated with dreaming.
Activation of the cortex is dependent on stimulation from cholinergic and adrenergic (using the neurotransmitters acetylcholine and norepinephrine) fibers in the ascending reticular activating system.
These fibers arise from the midbrain reticular formation and the tegmentum, travel to the intralaminar nucleus of the thalamus, through the internal capsule, and to the cortex bilaterally.
The specific ability to be aware of oneself involves higher cognitive functions as well. I happen to believe that the subjective experience of consciousness is the result of multiple parallel processes, but this is not fully understood.
Of course, consciousness can be altered in multiple ways.
1) Barbituate overdose. Barbituate drugs stimulate a neurotransmitter receptor for GABA (gamma aminobutryic acid). When stimulated, this receptor causes an induction of chloride into the cell, making the electrochemical gradient more negative, hyperpolarizing the cell, and decreasing its ability to undergo an action potential and stimulate other neurons. In other words, it is a central nervous system depressant. Many other drugs (opiates, alcohol, etc) share this property. The result is a depression of consciousness and even a comatose state in severe overdose. In high enough doses, the medullary respiratory center cannot function, and the patient will die of respiratory failure. The drug also causes slowing of the electrical activity in the brain, and it can prevent normal unconscious brainstem evoked responses to stimuli. For instance, in unconscious individuals who are not brain dead, it is possible to induce electrical activity in the brain by stimulating the patient with sound (auditory brainstem evoked response, ABER). CNS depressant drugs can suppress this normal response.
2) Brain death.
In severe neurological injury (intracranial hemorrhage, brain herniation, penetrating brain injury, and so forth), the brain ceases to function. The patient may be kept alive on a mechanical ventilator (the medullary respiratory center controls breathing and is nonfunctioning in brain death), but the patient is completely comatose, does not respond to stimuli, cannot initiate breathing, and lacks cranial nerve reflexes.
So what happens when you die?
Lets say, for example, that you die of a cardiac arrest. Your heart stops beating, and your blood pressure drops to zero. You are no longer moving blood through your body which normally carries oxygen and nutrients to your bodys tissues. Your tissues are still metabolically active, and they quickly deplete the adenosine triphosphate substrate which is present.
Neurons happen to be essentially entirely dependent on aerobic respiration to replete ATP. Without ATP, they cannot maintain the sodium potassium pump which normally keeps the majority of potassium inside of the cell and the majority of sodium outside of the cell. Lacking this gradient, many of the normal functions of the cell cannot be carried out. Pathologically, this leads to a calcium influx into the cell, blebing of the cell membrane, activation of various caspase systems, and eventual necrosis of the cell.
In other words, the neurons die, and all of the functions discussed above relating to consciousness can no longer occur. Death of the cell in this manner is irreversible, just as death of brain tissue in a completed stroke is irreversible.
It is unclear exactly when this happens because the patient has long been unconscious, but we know it happens because we can see it under the microscope. Dead patients dont have organized neuroelectrical activity. They dont have brainstem auditory evoked responses.
In some instances, patients are successfully resuscitated after a cardiac arrest. Blood circulation is restored, and they once again receive oxygen and nutrients. If the resuscitation occurred quickly, the patient may have no neurological problems, but if there is prolonged cardiac arrest, the patient may have memory/personality changes, more severe neurological deficits, or even end up in a persistent vegetative state. There are rare cases of cardiac arrests occurring with hypothermia where patients recover completely even after prolonged arrest (because hypothermia slows down cell metabolism and delays irreversible damage).
If no resuscitation occurs, your neurons will die, and everything that you ever were your personality, your intelligence, your memory is gone forever. Albert Einsteins knowledge of physics and Bob Hopes brilliant wit were destroyed in minutes.
It is not impossible to posit an alternative reality. You could conjecture, for instance, that there exists a non-material substance like a soul or a spirit which contains a copy of your brain which does not require oxygen and nutrients and thus persists after death. Aside from the lack of evidence in favor of this proposition, there are various theoretical problems with it.
Lets say you die, and your soul goes to heaven. Which aspect of your consciousness does your soul contain? You are constantly changing. If you acquire a severe dementia prior to death such that you were unable to remember your own name, are you still demented in the afterlife or being resistant to physical damage, does your soul have the memory of a younger version of yourself? If you acquire a physical disability during life such as blindness, does your soul have similar limitations? Everyone acquires catastrophic neurological injury at the time of death (see above), so a soul that simply mirrored the body would be useless. What if you had cerebral palsy and lived your entire life with severe mental and physical disabilities? Does your soul, being resistant to physical injury, make you a person in the afterlife that you never were during life? How would your soul have sensation anyways? Sensation is necessarily dependent on matter; for instance, vision depends on a matter being influenced by electromagnetic radiation.
This is all, of course, nonsense. Why would we posit an entirely new form of substance simply to pretend that we can cheat death. Its a gross violation of Occams razor.
It may be nice to believe that you will live forever. It may make you feel warm and fuzzy when you go to sleep at night. However, my advice is live it up and do great things because this is the only life you get
enjoy
--------
Consciousness is the feature of self-awareness, the ability to perceive sensation, and the ability to think. It is often characterized as having an emotional state and internal volition.
My central point is that the mind is a direct manifestation of the physical brain.
That is, all of sensation, emotion, perception, thought, memory, personality, self awareness, and volition is a result of the properties of the gelatinous organ between your ears.
Allow me to build my case by providing a large number of examples from clinical neurology. This may seem somewhat tedious, but I am trying to develop the idea that the mind is not a black box. It is quite well understood, and there is no longer any need to guess at its functions. I am attempting to give specific detailed examples. My format is 1) sensory modality, 2) anatomy (where it is located in the brain), 3) pathology (how it is destroyed in disease states)
Sensation:
vibration sensation of the skin:
vibration is sensed by small organs called pacinian corpuscles in the skin. Information is carried through large myelinated fibers to the dorsal column, the medial lemniscus, the ventral posterolateral nucleus of the thalamus, and ultimately to the contralateral primary somatosensory cortex.
Destruction of any of these areas leads to a loss of vibration sensation.
examples:
1) The dorsal column in syphilis
2) The somatosensory cortex in middle cerebral artery stroke
vision:
The electromagnetic stimulation of light is translated into an electrochemical signal in the rods and cones in the retina which is ultimately transferred to bipolar cells and then ganglion cells whose axons converge to form the optic nerve, the optic chiasm, the optic tract...and ultimately synapse in the primary visual cortex (Brodmann's area 17) which interacts with association areas in complex ways.
Damage to various components of the visual system can cause different consequences
examples:
1) macular degeneration can cause distortion of visual images (though accumulation of drusen in the retina)
2) Compresion of the optic chiasm by a pituitary adenoma (a tumor of the pituitary gland) can cause tunnel vision (bitemporal hemianopia).
3) A stroke in the posterior cerebral artery can cause loss of vision to one side (homonymous hemianopia) with sparing of central vision (macular sparing)
4) brain tumors in the occipitotemporal area can (rarely) cause the inability to recognize complex objects or even specifically the ability to recognize faces (aprosopagnosia). This is related to the inability to process and interpret complex visual data.
This all likely comes off as being esoteric and turgid. That is not my intention. My intention is to emphasize how well understood neurology is. Of course...you would never question me on this. You know that vibration sensation and vision are organic phenomena which are purely the result of the physical brain. They do not require supernatural explanations. They do not require a soul or a spirit to work. The argument which I am making is that these aspects of consciousness are perhaps more well understood but no less supernatural than other aspects of consciousness. Allow me to continue.
memory:
Memory involves the linking of various areas of the brain and changing of the properties of synaptic connections
it is mediated to a large extent by the papez circuit below:
complex information from all aspects of the nervous system enter the subiculum of the hippocampus from the parahippocampal gyrus and entorhinal cortex. The hippocampus itself is responsible for the formation of the new circuits. This is believed to occur through upregulation of glutamate receptors (glutamate is an excitatory neurotransmitter) so that a new or modified ability of one neuron to act on another is created. This information is then relayed to the cingulate gyrus which is responsible for much of the emotional significance or emotional content of memory.
Note: Different forms of memory are believed to be formed in different ways. For example, the cerebellum plays a large role in memory of fine procedural coordination (motor memory)
Memory can be altered in various ways clinically.
1) Simple amnestic seizure. In very rare cases, a seizure in the hipocampus on the dominant side can cause amnesia for the time period while the seizure is occurring with no other symptoms.
2) Transient global amnesia. this a rare syndrome where a patient loses the ability to form new memories for several hours. The patient often repeats questions over and over and then recovers completely. Some of these cases are believed to be due to poor venous drainage from the hippocampus.
3) korsakoff's syndrome-this is caused by vitamin B1 (thiamine) deficiency often seen in alcoholics which leads to bilateral hemorrhage and destruction of the mamillary bodies (see diagram above). The result is a permanent inability to form new memories (similar to the protagonist in the movie Memento)
4) In the past, it was common to perform a temporal lobectomy (removal of the temporal lobe) in patients with seizure disorders to control seizures. This would very commonly lead to severe defects in spatial memory.
5) In Alzheimers dementia, amyloid plaques accumulate in cells, leading to neuronal death, particularly in the temporal and frontal lobes. This initially causes short term memory difficulties and ultimately profound amnesia.
emotion:
Surely, emotion is a complex phenomenon. Much of emotion is believed to be related to the interaction of the limbic system. Here are some pieces of the puzzle:
The anterior nucleus of the thalamus receives the mamillothalamic tract and projects to the cingulate gyrus, linking memory with the main gyrus which regulates emotion.
The amygdala (which lies adjacent to the parahippocampal gyrus) causes fear and a sort of "fight or flight" response when stimulated (in addition to the anterior nucleus of the hypothalamus).
The nucleus accumbens is located in the basal ganglia and contains many dopaminergic neurons (neurons which use dopamine as a neurotransmitter). It has a known involvement in pleasure, reward, addiction, and the placebo effect.
Clinical correlates
1) The herpes virus can rarely cause an encephalitis (brain inflammation) syndrome which can cause destruction of the amygdala. This can lead to what is known as "kluver bucy syndrome." Patients with this syndrome are extremely placid. They lose their normal responses of fear and anger to stimuli, and they exhibit unusual improper sexual behavior (such as indiscriminately trying to have sex with inanimate objects)
2) abnormalities in the serotonin producing neurons in the raphe nuclei and norepinephrine producing neurons in the locus ceruleus are believed to be related to symptoms of depression and anxiety, and various drug treatments target these receptors.
3) Pleasure causing drugs such as heroin indirectly cause increased dopaminergic release in the nucleus accumbens which causes the sensation of incredible euphoria. Prolonged stimulation can cause downregulation of the dopamine receptors which can lead to physical dependence, anhedonia during withdrawal, and drug addiction
Personality:
Some aspects of personality are related closely with other systems (see kluver bucy syndrome). However, personality is dependent not only on deep seated nuclei in the brain (the amygdala, the cingulate gyrus, etc.) but also the more rostral structures such as the prefrontal cortex. These areas are also related to "higher" thought processes such as judgment, planning, morality, and logic. I'll simply discuss some cases.
1) There is a very famous case of a man named Phineas P. Gage who worked as a railroad construction foreman during the 19th century. He was injured by a large iron rod which was driven through the front of his skull, destroying much of his frontal lobe. After the event, he had an excellent recovery. However, he was noted by his peers to have various personality changes. He was childish, profane, and disinhibited on some accounts.
2) The procedure known as frontal lobotomy (destruction of the frontal lobe) was performed in a large number of patients for various psychiatric problems in the early 20th century. Destruction of the right frontal lobe would at times induce mania in depressed individuals. Destruction of the left frontal lobe would at times cause apathy or resolution of mania in the angry or manic patient respectively.
3) There are cases of right frontal lobe strokes and tumors which cause mania. Left frontal lobe stroke is associated with severe depression.
Self awareness:
Various experiments have determined that alertness, ability to process information, and reaction to stimuli is dependent on activity of the cortex (the surface) of the brain. There are various intermediate states of consciousness which occur during sleep or occur on a subconscious level, but all of these require activation of the cortex. Patients who are brain dead, for instance, do not exhibit sleep cycle changes associated with dreaming.
Activation of the cortex is dependent on stimulation from cholinergic and adrenergic (using the neurotransmitters acetylcholine and norepinephrine) fibers in the ascending reticular activating system.
These fibers arise from the midbrain reticular formation and the tegmentum, travel to the intralaminar nucleus of the thalamus, through the internal capsule, and to the cortex bilaterally.
The specific ability to be aware of oneself involves higher cognitive functions as well. I happen to believe that the subjective experience of consciousness is the result of multiple parallel processes, but this is not fully understood.
Of course, consciousness can be altered in multiple ways.
1) Barbituate overdose. Barbituate drugs stimulate a neurotransmitter receptor for GABA (gamma aminobutryic acid). When stimulated, this receptor causes an induction of chloride into the cell, making the electrochemical gradient more negative, hyperpolarizing the cell, and decreasing its ability to undergo an action potential and stimulate other neurons. In other words, it is a central nervous system depressant. Many other drugs (opiates, alcohol, etc) share this property. The result is a depression of consciousness and even a comatose state in severe overdose. In high enough doses, the medullary respiratory center cannot function, and the patient will die of respiratory failure. The drug also causes slowing of the electrical activity in the brain, and it can prevent normal unconscious brainstem evoked responses to stimuli. For instance, in unconscious individuals who are not brain dead, it is possible to induce electrical activity in the brain by stimulating the patient with sound (auditory brainstem evoked response, ABER). CNS depressant drugs can suppress this normal response.
2) Brain death.
In severe neurological injury (intracranial hemorrhage, brain herniation, penetrating brain injury, and so forth), the brain ceases to function. The patient may be kept alive on a mechanical ventilator (the medullary respiratory center controls breathing and is nonfunctioning in brain death), but the patient is completely comatose, does not respond to stimuli, cannot initiate breathing, and lacks cranial nerve reflexes.
So what happens when you die?
Lets say, for example, that you die of a cardiac arrest. Your heart stops beating, and your blood pressure drops to zero. You are no longer moving blood through your body which normally carries oxygen and nutrients to your bodys tissues. Your tissues are still metabolically active, and they quickly deplete the adenosine triphosphate substrate which is present.
Neurons happen to be essentially entirely dependent on aerobic respiration to replete ATP. Without ATP, they cannot maintain the sodium potassium pump which normally keeps the majority of potassium inside of the cell and the majority of sodium outside of the cell. Lacking this gradient, many of the normal functions of the cell cannot be carried out. Pathologically, this leads to a calcium influx into the cell, blebing of the cell membrane, activation of various caspase systems, and eventual necrosis of the cell.
In other words, the neurons die, and all of the functions discussed above relating to consciousness can no longer occur. Death of the cell in this manner is irreversible, just as death of brain tissue in a completed stroke is irreversible.
It is unclear exactly when this happens because the patient has long been unconscious, but we know it happens because we can see it under the microscope. Dead patients dont have organized neuroelectrical activity. They dont have brainstem auditory evoked responses.
In some instances, patients are successfully resuscitated after a cardiac arrest. Blood circulation is restored, and they once again receive oxygen and nutrients. If the resuscitation occurred quickly, the patient may have no neurological problems, but if there is prolonged cardiac arrest, the patient may have memory/personality changes, more severe neurological deficits, or even end up in a persistent vegetative state. There are rare cases of cardiac arrests occurring with hypothermia where patients recover completely even after prolonged arrest (because hypothermia slows down cell metabolism and delays irreversible damage).
If no resuscitation occurs, your neurons will die, and everything that you ever were your personality, your intelligence, your memory is gone forever. Albert Einsteins knowledge of physics and Bob Hopes brilliant wit were destroyed in minutes.
It is not impossible to posit an alternative reality. You could conjecture, for instance, that there exists a non-material substance like a soul or a spirit which contains a copy of your brain which does not require oxygen and nutrients and thus persists after death. Aside from the lack of evidence in favor of this proposition, there are various theoretical problems with it.
Lets say you die, and your soul goes to heaven. Which aspect of your consciousness does your soul contain? You are constantly changing. If you acquire a severe dementia prior to death such that you were unable to remember your own name, are you still demented in the afterlife or being resistant to physical damage, does your soul have the memory of a younger version of yourself? If you acquire a physical disability during life such as blindness, does your soul have similar limitations? Everyone acquires catastrophic neurological injury at the time of death (see above), so a soul that simply mirrored the body would be useless. What if you had cerebral palsy and lived your entire life with severe mental and physical disabilities? Does your soul, being resistant to physical injury, make you a person in the afterlife that you never were during life? How would your soul have sensation anyways? Sensation is necessarily dependent on matter; for instance, vision depends on a matter being influenced by electromagnetic radiation.
This is all, of course, nonsense. Why would we posit an entirely new form of substance simply to pretend that we can cheat death. Its a gross violation of Occams razor.
It may be nice to believe that you will live forever. It may make you feel warm and fuzzy when you go to sleep at night. However, my advice is live it up and do great things because this is the only life you get