You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Do failed MILD, Vertiflex, and Minuteman count as FBSS in SCS Algorithm?
Started by drusso

What did I just read?
Interesting thought. Microdiscectomy certainly counts, so does endoscopic? Percutaneous? Where is the line drawn?
there i$ no line if the denominator i$ reimbur$ement from the$e procedure$
there i$ no line if the denominator i$ reimbur$ement from the$e procedure$
Can you elaborate what you mean?
I gotta remember this thread for the next big Medicare fraud bust on stimulators
Do you think stim is over-utilized?
When I do it? No.Do you think stim is over-utilized?
Is there a guy across the road who puts his stim in you on the first date? Yes. And then gets all creepy on you to get the permanent when the stim didn't help? Yes yes. I've gotten a couple of older patients who let their batteries die because "it never helped in the first place." It's not a stretch to imagine someone inappropriately calling interspinous spacer placement FBSS because it benefits their interests.
When I do it? No.
Is there a guy across the road who puts his stim in you on the first date? Yes. And then gets all creepy on you to get the permanent when the stim didn't help? Yes yes. I've gotten a couple of older patients who let their batteries die because "it never helped in the first place." It's not a stretch to imagine someone inappropriately calling interspinous spacer placement FBSS because it benefits their interests.
"Over-utilizer" = "Anyone who does more ________ than me?"
Advertisement - Members don't see this ad
Seen it. Several times. Usually combo of Vertiflex or some other variant, then SI fusions by pain dr. Failed? Fbss. Scs. Then come to me for 2nd opinion. Typically 50-70 with severe stenosis. Off to surgeon you go.Drusso, are you trying to play devils advocate here or are you asking for permission? If someone puts a spacer in a virgin spine and then tells them they failed surgery, that’s shady.
Drusso, are you trying to play devils advocate here or are you asking for permission? If someone puts a spacer in a virgin spine and then tells them they failed surgery, that’s shady.
I'm just trying to stoke some grown-up conversation around here...who decides who fails what? The patient, the treating doctor, or a second opinion?
Should the stim come first or second in "the algorithm?"
We can go back to talking about meth-head fish?
Last edited:
You cant do scs until youve done at least two 150k back fusions and the patient can’t walk.. everyone knows that.
Last edited:
We all know Lou is ready to put a Wavewriter Alpha in that Vflex patient, but looks like he did a very good job on the vflex. There are nice neuroforamenal openings at the treated levels and the levels above and below. I would expect
that patient to do very well. There is nothing to criticize there.
that patient to do very well. There is nothing to criticize there.
Approval guidelines usually require that there is no corrective surgery or that patient is not a good candidate for it, which is subjective.
Many older stenotic patients are not good candidates for lami/fusion so I think SCS after failure of mild or Vflex is appropriate in this population. There was a thread on here about this before.
Many older stenotic patients are not good candidates for lami/fusion so I think SCS after failure of mild or Vflex is appropriate in this population. There was a thread on here about this before.
the guiding principle of some of our thought leaders is that procedures that generate significant financial reward are the treatments we need to be advocating and performing.Can you elaborate what you mean?
I rarely see these leaderss advocating for treatments that, for example, your wife provides. maybe a passing "oh they get a referral for CBT in our office"...
there are at least 3 separate "pain" programs in this area that are run as block shops. id guestimate almost all of my private pay referrals are from patients who have gone to these other practices where the first and only time they see the pain doctor is in Pre An.
yes, these are the successful (financially) programs in town. 1 of the 3 is private.
the guiding principle of some of our thought leaders is that procedures that generate significant financial reward are the treatments we need to be advocating and performing.
I rarely see these leaderss advocating for treatments that, for example, your wife provides. maybe a passing "oh they get a referral for CBT in our office"...
there are at least 3 separate "pain" programs in this area that are run as block shops. id guestimate almost all of my private pay referrals are from patients who have gone to these other practices where the first and only time they see the pain doctor is in Pre An.
yes, these are the successful (financially) programs in town. 1 of the 3 is private.
How does CBT fix stenosis?
does SCS fix stenosis?
does vertiflex or minuteman or MILD actually fix stenosis?
does vertiflex or minuteman or MILD actually fix stenosis?
Advertisement - Members don't see this ad
does SCS fix stenosis?
does vertiflex or minuteman or MILD actually fix stenosis?
I'd be pissed if you told me my claudication was caused by my "stinking thinking."
aside from the continuous lack of any collimationWe all know Lou is ready to put a Wavewriter Alpha in that Vflex patient, but looks like he did a very good job on the vflex. There are nice neuroforamenal openings at the treated levels and the levels above and below. I would expect
that patient to do very well. There is nothing to criticize there.
Tell me more about tour anger issues.I'd be pissed if you told me my claudication was caused by my "stinking thinking."
My dad never told me he loved me or that he was proud of me.Tell me more about tour anger issues.
D
deleted875186
I think in the future SCS will be more available to surgically naive patients, I’m sure Medtronic and others are working on the study.
DPN. Nevro. Excited to tear apart the study SIS.I think in the future SCS will be more available to surgically naive patients, I’m sure Medtronic and others are working on the study.
yes the truth hurts sometimes.I'd be pissed if you told me my claudication was caused by my "stinking thinking."
or most of the time.
so lets just hide behind a veneer of big arse procedures or mind altering substances.
D
deleted875186
I don’t think SCS should be used for every neuropathic pain condition like it’s a holy grail.DPN. Nevro. Excited to tear apart the study SIS.
but if we put in stims for FBSS, who’s to say a lot of the chronic radic and back pain that is surgically naive wouldn’t benefit, just can’t predict who is going to have persistent pain after surgery.
yes the truth hurts sometimes.
or most of the time.
so lets just hide behind a veneer of big arse procedures or mind altering substances.
If there is one lesson physicians should have learned in the 20th century is that the misattribution of neurological symptoms to psychiatric disease is almost always wrong: See MS, schizophrenia, depression, anxiety, autism, etc for examples.
Treat all pain and pain treatment failures as biological problems until proven otherwise.
That’s a terrible idea. Pain is a symptom and not a disease.If there is one lesson physicians should have learned in the 20th century is that the misattribution of neurological symptoms to psychiatric disease is almost always wrong: See MS, schizophrenia, depression, anxiety, autism, etc for examples.
Treat all pain and pain treatment failures as biological problems until proven otherwise.
Advertisement - Members don't see this ad
That’s a terrible idea. Pain is a symptom and not a disease.
Chronic pain as a symptom or a disease: the IASP... : PAIN
nvestigations difficult and impedes health policy decisions regarding chronic pain such as adequate financing of access to multimodal pain management. In cooperation with the WHO, an IASP Working Group has developed a classification system that is applicable in a wide range of contexts...
 journals.lww.com
journals.lww.com
so every patient gets opioids, because from most patients standpoint that is the treatment for a biological problem.If there is one lesson physicians should have learned in the 20th century is that the misattribution of neurological symptoms to psychiatric disease is almost always wrong: See MS, schizophrenia, depression, anxiety, autism, etc for examples.
Treat all pain and pain treatment failures as biological problems until proven otherwise.
can you rightly say that scrambling central nervous system pathways benefits any of those conditions? is frontal lobotomy the treatment of choice for MS, schizophrenia, depression, anxiety, autism?
Chronic pain as a symptom or a disease: the IASP... : PAIN
nvestigations difficult and impedes health policy decisions regarding chronic pain such as adequate financing of access to multimodal pain management. In cooperation with the WHO, an IASP Working Group has developed a classification system that is applicable in a wide range of contexts...
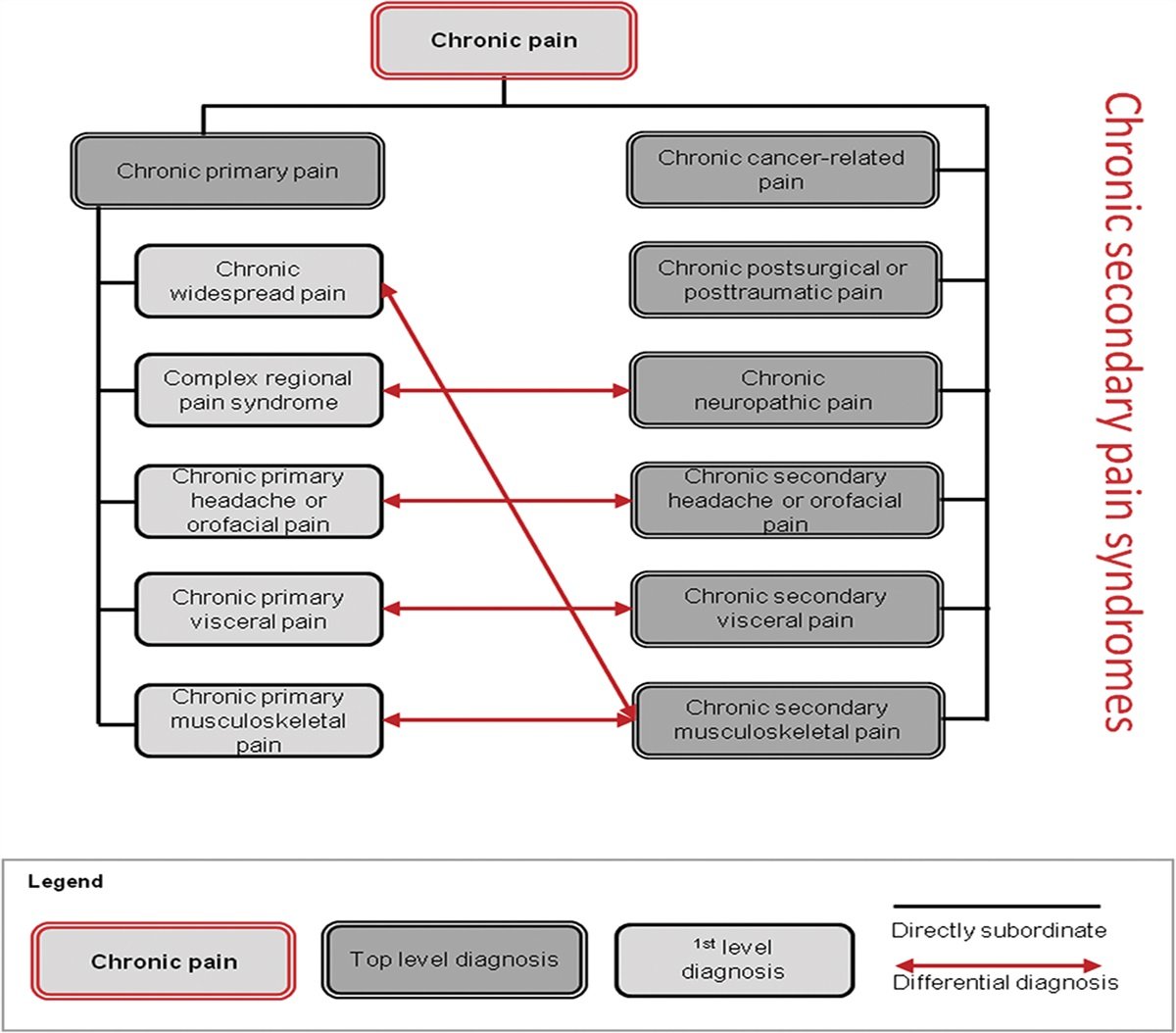
not sure how that makes your point that pain as a separate specific disease. essentially, this working group wants fibromyalgia and nonspecific low back pain to be classified as a separate disease called "chronic primary pain" and other pain syndromes that are associated with a disease to be called "chronic secondary pain", each with its own ICD. the purpose is to facilitate epidemiologic studies and change health policies and I'm not seeing anything about a true biological basis for making this classification.
What duct said. They aren’t arguing it is a disease. Just a title to draw attention and try and score research $$$$Chronic pain as a symptom or a disease: the IASP... : PAIN
nvestigations difficult and impedes health policy decisions regarding chronic pain such as adequate financing of access to multimodal pain management. In cooperation with the WHO, an IASP Working Group has developed a classification system that is applicable in a wide range of contexts...
What duct said. They aren’t arguing it is a disease. Just a title to draw attention and try and score research $$$$
@Ducttape and @lobelsteve ganging up on @drusso...there is a disturbance in The Force...
I also agree, financials aside, that people should have the option of SCS without needing someone cutting their spine first.
not ganging up.... but you are man enough to take it.@Ducttape and @lobelsteve ganging up on @drusso...there is a disturbance in The Force...
we already have enough inappropriate use of advanced procedures. if we were to give the option to do SCS without prior surgery, there need to be some appropriate indications that are fairly strict. otherwise the success rate will continue to plummet...I also agree, financials aside, that people should have the option of SCS without needing someone cutting their spine first.
(some of the outstanding inappropriate uses I have personally seen in past - ITP for atypical facial pain; ITP for healed compression fx that failed tramadol; lumbar SCS for cervical postlaminectomy; SCS in nonsurgical normal spine and no neuropathy sx; cervical SCS for total body CRPS)
No one is gangin up on you, just on that article published to garner research dollars. We appreciate you posting it.@Ducttape and @lobelsteve ganging up on @drusso...there is a disturbance in The Force...
I’ve done plenty of successful stim in old folks that refuse surgery or are poor candidates for major interventions. It’s a good option for the over 80 year olds that I see
Old folks can do really well. ABT set it snd forget it.
Advertisement - Members don't see this ad
Just make the reimbursement $500, inappropriate use would stop.not ganging up.... but you are man enough to take it.
we already have enough inappropriate use of advanced procedures. if we were to give the option to do SCS without prior surgery, there need to be some appropriate indications that are fairly strict. otherwise the success rate will continue to plummet...
(some of the outstanding inappropriate uses I have personally seen in past - ITP for atypical facial pain; ITP for healed compression fx that failed tramadol; lumbar SCS for cervical postlaminectomy; SCS in nonsurgical normal spine and no neuropathy sx; cervical SCS for total body CRPS)