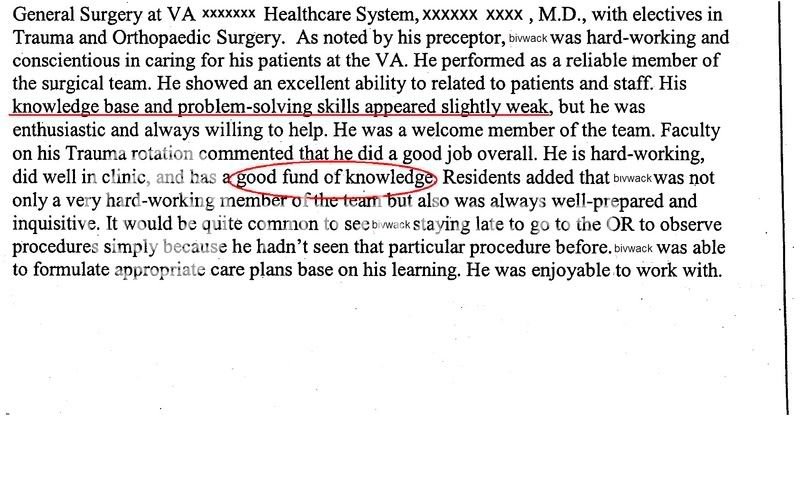
Wondered about the fund of knowledge eval. It seemed to appear in several threads I read on SDN. I thought I understood what it meant, but maybe not.
I know evals are very unpredictable but I've seen where I have answered minimal questions and recieved " good fund of knowledge" on my evals and other times I've worked my butt off answered 85- 90 correct and recieved low fund of knowledge. Go figure. But Idid honered in my chosen field.
Is the fund of knowlege eval a general statement like needs to read more?
Is fund of knowlege refering to book info or patient into or treatment??? Just wondered if this eval continues in internship year and residency?
I know evals are very unpredictable but I've seen where I have answered minimal questions and recieved " good fund of knowledge" on my evals and other times I've worked my butt off answered 85- 90 correct and recieved low fund of knowledge. Go figure. But Idid honered in my chosen field.
Is the fund of knowlege eval a general statement like needs to read more?
Is fund of knowlege refering to book info or patient into or treatment??? Just wondered if this eval continues in internship year and residency?