- Joined
- Jul 22, 2011
- Messages
- 64
- Reaction score
- 11
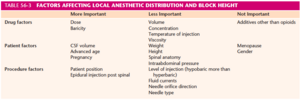
Hey, anyone look at the patient height when it comes to how much Bupivacaine to put in the spinal or does everyone put 10.5 mg and 12 mg?
yes. 1.6 -1.8 ml depending on heightHey, anyone look at the patient height when it comes to how much Bupivacaine to put in the spinal or does everyone put 10.5 mg and 12 mg?
If they're getting through without you needing to support with IV meds, then you're not underdosing.Wow. I must be underdosing a lot then. I’ve done 1-1.5 ml of 0.75%. All those with fent and duramorph. Some of the ob’s where I trained, regular c-section is half hour.
Watch the glass spine videos on youtubeOut of curiosity, let say you have someone that 5’2” and you put Bupivacaine 12mg, Fentyl 15 mcg and Duramorph 0.2 mg, do you put the the patient reverse Tberg to prevent the spinal from going to high
Never done such a thing. If their fingers start tingling, it's perfect.Out of curiosity, let say you have someone that 5’2” and you put Bupivacaine 12mg, Fentyl 15 mcg and Duramorph 0.2 mg, do you put the the patient reverse Tberg to prevent the spinal from going to high
Out of curiosity, let say you have someone that 5’2” and you put Bupivacaine 12mg, Fentyl 15 mcg and Duramorph 0.2 mg, do you put the the patient reverse Tberg to prevent the spinal from going to high
Hey, anyone look at the patient height when it comes to how much Bupivacaine to put in the spinal or does everyone put 10.5 mg and 12 mg?
Someone please correct me if I'm wrong, but I recall being told in fellowship that there's no data to support dose reductions / increases to account for extremes in height. Now whether that was in the context of a isobaric vs hyperbaric discussion I can't recall, but I took from that discussion to mean all baricities. That being said, just the other day I gave 12 mg of hyperbaric bupi to a patient who's 4'11" without any problems. Level was just under T5/6. I normally don't check levels but in this case I was curious.
To address the topic here, I think volume is much more important than actual bupi dose (to some degree oc). I have partners that get away with 9 mg of Bupi, but put 20 mcg of fent and 0.2 mg of duramorph. That equates to about 1.8 cc volume. I do 12 mg of bupi, 0.1 mg duramorph, and 10 mcg Fent which equates to 1.9 cc. I've had partners attempt 9 mg bupi, no fent, and 0.1 duramorph (1.3 cc) with levels that failed Allis and required redosing. I of course would never test this, but I think had they just increased the volume with saline it would have spread high enough to be effective.
Ultimately, what are we gaining by limiting the dose of Bupi for "fast" surgeons? Is it that uncomfortable for patients to have an effective spinal for 30-45 minutes longer with a higher dose that's guaranteed not to "fail"? People will often cite the hypotension and n/v as a reason to limit the dose, but I have no issues with this by infusing phenylephrine proactively instead of being reactionary to the symptoms of hypotension.
Thoroughly enjoyed learning from Dr Gaiser. 15mg for everyone. “When they ask you on oral boards what your dose is, paused and act like you’re really contemplating the situation, then just say 15mg.”15mg for everyone at my exceptionally slow institution. 2+hr c-sections on the regular. This was taught to me by Bob Gaiser, a very prominent physician in OB anesthesia. Obviously if we had fast OBs, I'd adapt.
Edit: just to add, these also get 15mcg fentanyl and 150mcg duramorph.
Someone please correct me if I'm wrong, but I recall being told in fellowship that there's no data to support dose reductions / increases to account for extremes in height. Now whether that was in the context of a isobaric vs hyperbaric discussion I can't recall, but I took from that discussion to mean all baricities. That being said, just the other day I gave 12 mg of hyperbaric bupi to a patient who's 4'11" without any problems. Level was just under T5/6. I normally don't check levels but in this case I was curious.
To address the topic here, I think volume is much more important than actual bupi dose (to some degree oc). I have partners that get away with 9 mg of Bupi, but put 20 mcg of fent and 0.2 mg of duramorph. That equates to about 1.8 cc volume. I do 12 mg of bupi, 0.1 mg duramorph, and 10 mcg Fent which equates to 1.9 cc. I've had partners attempt 9 mg bupi, no fent, and 0.1 duramorph (1.3 cc) with levels that failed Allis and required redosing. I of course would never test this, but I think had they just increased the volume with saline it would have spread high enough to be effective.
Ultimately, what are we gaining by limiting the dose of Bupi for "fast" surgeons? Is it that uncomfortable for patients to have an effective spinal for 30-45 minutes longer with a higher dose that's guaranteed not to "fail"? People will often cite the hypotension and n/v as a reason to limit the dose, but I have no issues with this by infusing phenylephrine proactively instead of being reactionary to the symptoms of hypotension.
I agree, the studies I've looked at however have shown mixed results. But the boards answer is still no difference.classic textbook knowledge would state that volume has little impact on block height for spinal. lack of fentanyl can decrease block duration and density though.
Should have clarified, my thought was in the context of using bupi for csections, so I have little motivation to time the spinal to the surgery. I generally haven't used Bupi for anything else these days. Isobaric Chloro/Mepi/Ropi covers pretty much everything else I do.And as for dropping the dose for fast surgeons, the only realistic reason is to move themeatpatient through pacu faster.
Should have clarified, my thought was in the context of using bupi for csections, so I have little motivation to time the spinal to the surgery. I generally haven't used Bupi for anything else these days. Isobaric Chloro/Mepi/Ropi covers pretty much everything else I do.
This. No epi though. I work in a community hospital and the skin to skin time is around 30-45mins.Roughly 1.4-1.8. Like <5'4 might get 1.4 if we know the surgeon is looking to be fast. Almost always putting duramorph, fent, epi anyway which seems to leave plenty of wiggle room.
PACU time.Ultimately, what are we gaining by limiting the dose of Bupi for "fast" surgeons? Is it that uncomfortable for patients to have an effective spinal for 30-45 minutes longer with a higher dose that's guaranteed not to "fail"? People will often cite the hypotension and n/v as a reason to limit the dose, but I have no issues with this by infusing phenylephrine proactively instead of being reactionary to the symptoms of hypotension.
Same.Ok. Yea, 99.9% of my C-sections get 12mg hyperbaric bupi. Don't care what OB is holding the scalpel.
Just say "One amp"Thoroughly enjoyed learning from Dr Gaiser. 15mg for everyone. “When they ask you on oral boards what your dose is, paused and act like you’re really contemplating the situation, then just say 15mg.”
Your sections go to PACU? At the institutions I've been at they always just go straight back to their L&D room where they're recovered by their nurse. Limiting the number of rocks in PACU is certainly an incentive to time the spinal to the surgery.PACU time.
If it's a slow surgeon who needs all day to get through 2 or 3 sections then it doesn't matter if the patient sits in PACU for 2 hours.
YesYour sections go to PACU? At the institutions I've been at they always just go straight back to their L&D room where they're recovered by their nurse. Limiting the number of rocks in PACU is certainly an incentive to time the spinal to the surgery.
Likewise.Yes
Maybe I've just been unlucky in the places I've worked, but I'd have some reservations about a floor L&D nurse watching an immediately-postop c-section patient.
My response was "how much is in the vial"Thoroughly enjoyed learning from Dr Gaiser. 15mg for everyone. “When they ask you on oral boards what your dose is, paused and act like you’re really contemplating the situation, then just say 15mg.”
For gods sake man does it really matter?So I have a scheduled primary C section for a lady that is 4’11” otherwise healthy. How much 0.75% Bupivicaine would you put in ? 1.4 ml or 1.6 ml ? It take the surgeon 1.0 hour to do the C section.
 Just flip a coin! If it's the higher dose and her fingers start to tingle, tilt the bed some!
Just flip a coin! If it's the higher dose and her fingers start to tingle, tilt the bed some!“Crash” c/s with spinal? No thanks.Dose should be adjusted based on gestational age (Kim H. Reg Anesth Pain Med 2019;44:793–795) and surgical time, not patient's height.
If surgery is ≤ 1 hr, 1.3 mL of 0.75% with Fentanyl should be enough. I've never had a problem with 1 mL for crash sections (25-30 minutes).
What dose you guys use if there is ****ty working epidural (meaning you'll take the catheter out and put a spinel) running at ~8–12 mL/hr)?
I would argue that when the indication is fetal distress without maternal issues a fast–track spinal doesn't really take much longer than a GA induction, in a patient with normal anatomy“Crash” c/s with spinal? No thanks.
I would argue that is fine if it is urgent but a true “crash” c/s is almost always a general, not a spinal.I would argue that when the indication is fetal distress without maternal issues a fast–track spinal doesn't really take much longer than a GA induction, in a patient with normal anatomy
Ohhh my apologies. Most of my anesthetic OB practice is in a different language. You're right, I meant urgent, not "crash".I would argue that is fine if it is urgent but a true “crash” c/s is almost always a general, not a spinal.