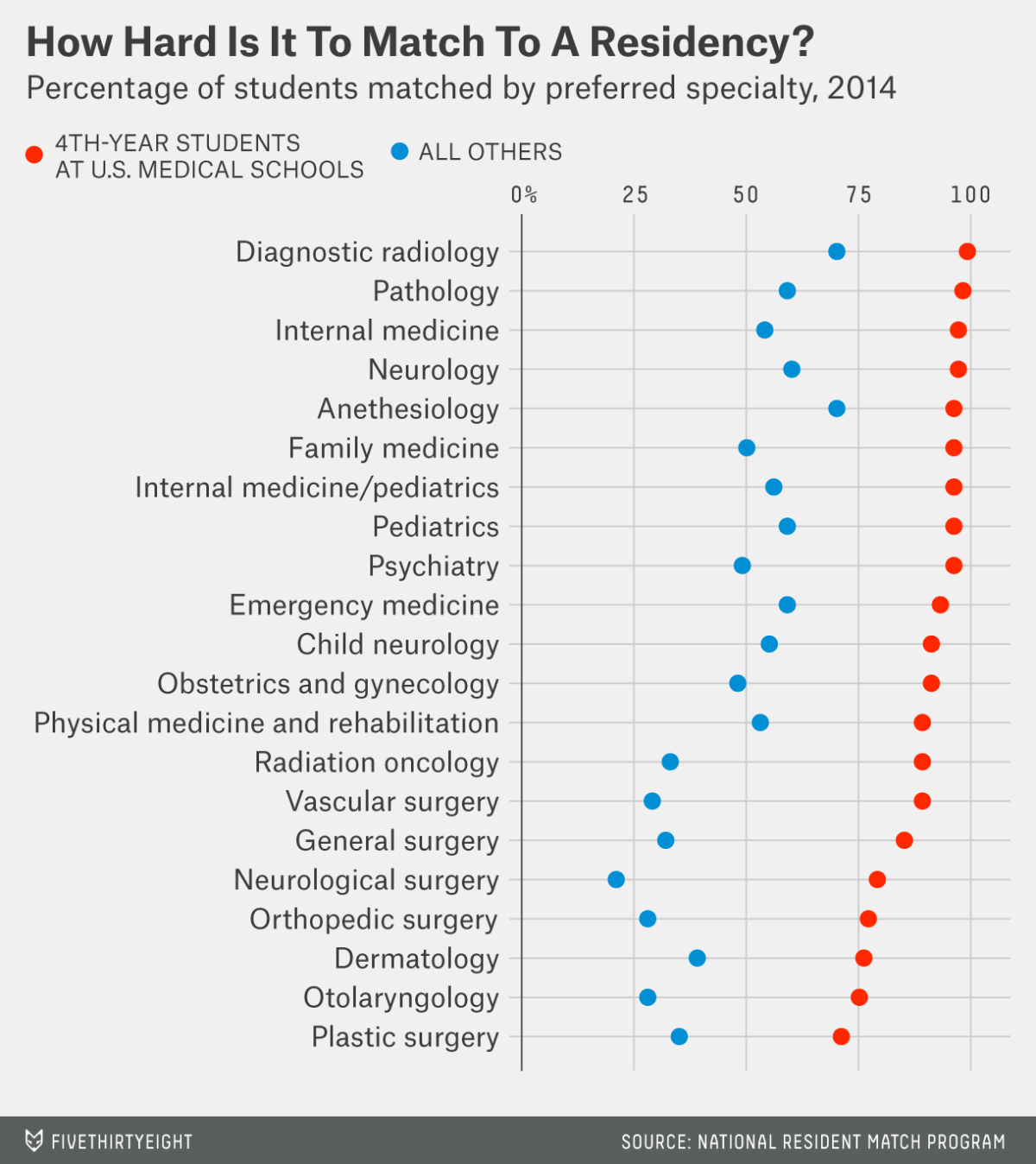
Last year, the NRMP showed that Plastic Surgery and ENT were some of the hardest fields to enter. Only about three-fourths of 4th year US medical students successfully matched into those programs. The numbers were even more abysmal for other students, like foreign medical graduates. They were able to get into those spots less than half the time.
By contrast, the least competitive programs had match rates of nearly 100%. For 2014, the surprising wallflower was Diagnostic Radiology. It was nearly impossible for future radiologists to not get into a radiology training program last year. Even FMG's had almost a 75% likelihood of matching into radiology.
While predictably Pathology and Internal Medicine were shunned by many medical students, look who rounded out the top five in the most unwanted residencies--Anesthesiology. It was actually easier to match into anesthesia than, horrors!, Family Medicine. This was especially true for FMG's, who had about a 75% chance of getting into anesthesia compared to 50% for Family Medicine.
Of course this shouldn't come as a surprise to anybody who's been paying attention. Demand for
anesthesiologists have been falling for some time now. The number of practicing anesthesiologists have increased at
twice the rate of the general population growth for the last decade. Meanwhile the anesthesia residency program directors keep cranking out more new graduates every year.
According to the NRMP, the number of PGY-1 spots in Anesthesiology has increased from 797 in 2010 to 1,049 last year.
The writing may be on the wall for the future of anesthesiologists. It is rapidly becoming a saturated medical specialty with too many providers scrambling for too few good jobs. Factor in the competition from non physicians, the anesthesia job market is on the verge of crashing under its own weight. Good luck to all the medical students on Match Day who want to go into Anesthesiology.
ZMD