- Joined
- Jan 31, 2009
- Messages
- 152
- Reaction score
- 49
Skin biopsy from the leg for bilateral lower extremity edema in an elderly female.

Check out a high power of my case (#50). And compare it to the pattern at low power....should help you classify this. Anybody know what stains to order??
For AutopsySweet's case (#51) I'm at intravascular lymphoma vs. carcinoma...would do a keratin and CD20 stain to start with...
Definitely an interesting and unexpected finding in what clinically probably looked like venous stasis!
Are we wrong about the Hodgkins?
You are correct about the Hodgkins! Just needed to load up the immuno's for you to see (CD15 and CD30). Called it mixed cellularity, given the architecture. Tricky case on low power though, since it focally involved the lymph node. You could easily blow by this node on low power as reactive with sinus histiocytes given the open sinuses....eeks!
Are we wrong about the Hodgkins?
Here is another case:
A 71 year old male with a tender skin nodule over his mastoid process.
Interesting, awesome case. I would actually have to see the slide for this and look at these cells closely. There doesn't seem to be an epidermal component as far as I can make out. There is alot of acute inflammation and the cells are certainly very atypical (I think they have nuclear inclusions) but I don't see any mitoses. I cannot completely rule out an infectious reactive process with all that acute inflammation.
I'd like a pan-CK, S100, HMB-45. 🙂
I don't have a PAS but I do have this:
As a bit of an aside to this thread, how was pathology performed before IHC? By that I mean a very high percentage of cases are only signed out after immunos, and tough cases basically get the kitchen sink. For those of you doing diagnostic path, do you find this good or bad? I think I'd have found it very frustrating, especially if working in a smaller setting without the availability of immunos most of us probably get accustomed to in residency.
Good thoughts everybody! Myeloid sarcoma/leukemia cutis as well as histiocytic lesions are definitely in the differential.
CD68 showed patchy dot-like cytoplasmic positivity in the cells of interest
View attachment 18238
CD1a is negative (although it can rarely be positive in this entity)
MPO, CD34, CD117/ckit, mast cell tryptase - all negative
BTW - does anyone have a preference for leaving the images attached so you have to click them open vs. inserting them directly into the post?
Bone marrow biopsy and aspirate for worsening anemia and hx of renal transplant.
Bone marrow biopsy and aspirate for worsening anemia and hx of renal transplant.
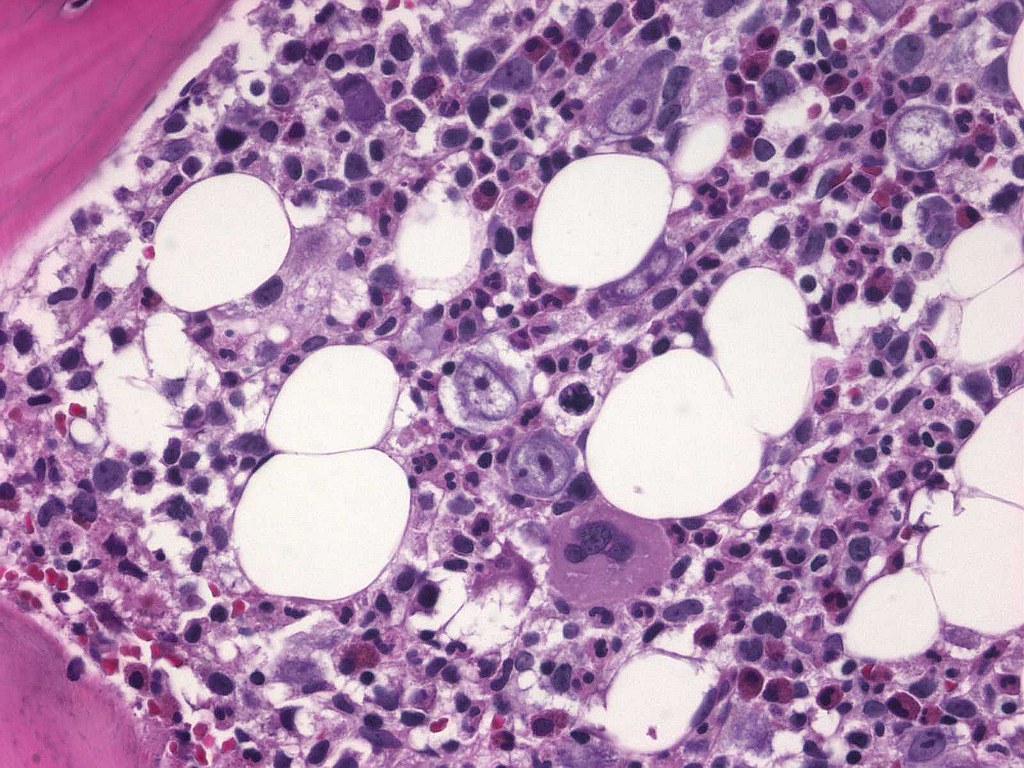
PCR was positive for parvovirus! Good job everyone 🙂 All the other cases so far have been great. Case #75 - what about CD 4, CD 8, and CD 56? How about CD4+/CD56+ hematodermic neoplasm?
PCR was positive for parvovirus! Good job everyone 🙂 All the other cases so far have been great. Case #75 - what about CD 4, CD 8, and CD 56? How about CD4+/CD56+ hematodermic neoplasm?
i'm sure that is what it is. WHO updated the name from agranular cd4+/cd56+ hematodermic neoplasm to blastic plasmacytoid dendritic cell neoplasm in 2008

WTG!!!
Blastic plasmacytoid dendritic cell neoplasm is correct. This case was positive for:
CD4
CD56
CD43
CD45 (LCA)
CD68 (in the dot-like pattern I showed before)
We also sent it out to get staining for CD123 and TdT (also positive)
Here is another case:
Abdominal mass in a 13 year old girl.
Here is another case:
Abdominal mass in a 13 year old girl.
here is another case:
Abdominal mass in a 13 year old girl.