- Joined
- Apr 16, 2004
- Messages
- 4,661
- Reaction score
- 5,080
I just saw this very interesting article on Medscape. Registration is free to read the article.
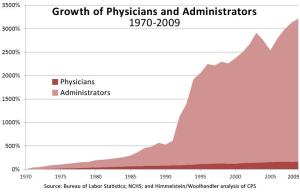
Rad Onc is not mentioned specifically as I'm sure the # of MDs is very small. However, it is interesting to see where the trends are going nationally.
Here are some choice quotes:
Rad Onc is not mentioned specifically as I'm sure the # of MDs is very small. However, it is interesting to see where the trends are going nationally.
Here are some choice quotes:
Within 2 years, more than 75% of newly hired physicians will be hospital employees, according to projections in a new report of physician recruiting incentives.
"Sixty-three percent of Merritt Hawkins' search assignments in 2011/12 featured hospital employment of the physician, up from 56 percent the previous year and only 11 percent eight years ago," the report states.
"Fewer doctors want to go into independent private practice," Phillip Miller, vice president of communications for Merritt Hawkins, told Medscape Medical News. "That's been a major trend over the past few years. The whole medical profession is shifting away from private practice to employment."
Demand for radiologists and anesthesiologists has decreased. Radiology, which was Merritt Hawkins' most requested specialty in 2003, ranked only 18th in 20112012. For the first time since the firm began compiling data, anesthesiology was not among its 20 most-requested search assignments.
"Anesthesiology is one of the few areas in medicine where allied health professionals, in this case certified registered nurse anesthetists, are replacing physicians," said Miller. "More states are allowing them to work unsupervised. Anesthesiology still attracts medical graduates and income is still attractive. But with the slumping economy, there are fewer elective procedures and that's having an impact.
"Radiologists also are affected by the economy," he adds. "As people put things off, there's less utilization. And compensation for radiologists has been cut by Medicare."