There are dual neurology/psychiatry programs some of which exist on a fluctuating basis but check out MUSC, Brown, NYU, Tulane, and UMass. It was unclear to me whether you are interested in treating neurological diseases (in which case you would need to train as a neurologist, not a psychiatrist) or if you were interested in the psychiatric aspects of neurology (in which case you could train as either a neurologist or psychiatrist).
If you are interested in the interface of neurology and psychiatry, then it is astounding that you are not interested in stroke or migraine! I am sure admitted strokes every 4th night would be quite tedious, stroke teaches us so much about brain-behavior correlates, the cerebral basis or mental disease, and creates some fascinating behavioral neurological symptoms. Strokes can result in depression, mania (usually right sided), and pseudobulbar affect. Strokes can lead to some of the most fascinating delusional syndromes including delusions of misidentification (chiefly the Capgras syndrome believed to result from disruption of the circuits between the fusiform facial gyrus and the amygala diminishing emotional response to faces and leading to the belief that an "imposter" has replaced loved ones), delusions of jealousy, erotomanic delusions, and delusions of infestation. Posterior circulation strokes can lead to peduncular hallucinations (vivid visual hallucinations that can be quite fantastical). I have seen patients develop obsessive compulsive disorder following strokes affecting the orbitofrontal cortex. Then there are the plethora of behavioral neurological syndromes that result from strokes including agnosias (including propasagnosia [inability to recognize faces], anosagnosia [inability to recognize deficits leading patients to behave as if they were normal], simultanagonsia[inability to see both parts and the whole]), apraxias, aphasias, aprosodia, amnesias. Posterior strokes can lead to Balint syndrome which is characterized by optic ataxia, optic ataxia, oculomotor apraxia and simultanagnosia. Whereas dominant parietal lobe lesions may lead to Gerstmann's syndrome which is characterized by dysgraphia, dyscalculia, finger agnosia, and left-right disorientation.
Then there are other rarities associated with strokes including foreign accent syndrome and the extremely rare le fou rire prodromique (uncontrollable fits of laughter that precede a catastrophic brainstem stroke/vascular event).
As for migraines, again they are simply fascinating neuropsychiatric occurrences! Migraine is in the differential diagnosis for psychosis, particularly of sudden onset. Persecutory delusions have been associated with the CACNL1A4 mutation which is a channelopathy cause of familial hemiplegic migraine. Distortions of time and space and sensory phenomena are quite classic of migraine. I have had patients describe distortions of the time-space continuum, or feel themselves completely disconnected from the universe during migraines. Oliver Sacks wrote about his amusia during migraines (i.e. the loss of sense of pitch and tone and inability to recognize familiar music). Olfacatory, visual, auditory hallucinations, illusions, synesthesia can all occur in migraine. There are even cases of foreign accent syndrome occuring with migraine; in
one case an english woman woke up sounding chinese! Migraines are eminently treatable and so it is very satisfying to make such a diagnosis in someone with more worrisome symptoms like delusions, hallucinations, blindness, hemiplegia etc.
a neuropsychiatry fellowship would give you absolutely no training in managing neurological diseases with the exception of the dementias.
As for DBS, it is not widely used in psychiatry because it is largely ineffective and insurance companies balk at paying for it in young people who will need the stimulator replaced several times. As you may be aware the last DBS depression trial (the BROADEN trial) was terminated by St Jude's Medical because it fared poorly on futility analysis. Currently OCD is the only psychiatric indication for DBS clinically, and that is not based on evidence, but a humanitarian device exception from the FDA because some cases of OCD are so catastrophic that patients (or their families) are desperate for surgery and DBS is by far the least worst surgical option. You could probably learn this during psychiatry residency if you worked with people who were doing this work or where they were clinically using DBS for OCD (I worked with a psychiatrist who did DBS programming when I was a resident). You could also do the interventional psychiatry fellowship at MUSC. I think Mt Sinai does a fair bit of research in this area too. I believe mayo has a brain stimulation fellowship they might be open to taking a psychiatrist. Personally, I think the main reason it's interesting doing this work is because of the fascinating treatment-refractory patients you evaluate and thinking through the management. your job as the psychiatrist is still primarily evaluation - there is nothing particularly fancy about fiddling with a DBS programming device though it is kinda cool at first the novelty wears off as with everything, and while it can sometimes be helpful the results are not typically dramatic (unlike in some movement disorders or epilepsy cases).
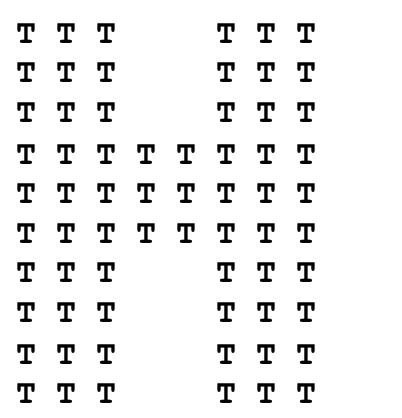
(patients with simultagnosia would see the T but not the H)
