Is anyone using the newer SNRI's for pain? results? papers?
Pristiq
Fetzima
Pristiq
Fetzima

thank You.Pain and psych here -- for some reason, Cymbalta seems to be the best. Effexor does help. I don't have much experience with Savella of Fetzima. Pristiq is excellent for depression/anxiety, but I haven't seen a profound difference in pain.
Is anyone using the newer SNRI's for pain? results? papers?
Pristiq
Fetzima
Are the agents effective because the patients clinical depression is improved and that reduces pain vs working on pain directly?Have not tried due to insurance limitations/cost for patient population
Reg Pristiq: Clinical experience with desvenlafaxine in treatment of pain associated with diabetic peripheral neuropathy
Did not see data on Fetzima
I rotate through them based on side effect profiles but I don't have experience with the newer ones enough to say. I have been slipping in some low dose Abilify and Zyprexa though to augment some of the usual agents with efficacy.
Cymbalta more noradrenergic than Savella? I was under the impression Savella did little serotonin and mostly NE.I would hardly call those new; Cymbalta is the most noradrenergic hence why the most pain benefit, however, they all have some pain benefit.
Cymbalta more noradrenergic than Savella? I was under the impression Savella did little serotonin and mostly NE.

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
I was a KOL for them. I can post my handouts when I get to my laptop.Nice Steve. I need to be as resourceful as you. I haven’t used Savella in a while but maybe I should revisit.
There should be generics based on age of drug. No one making it that I can see.Almost every savella script I’ve written has been denied by insurrance, probably going to give up even trying it.
Never used them. I recently starting trying savella for fibro patients, typically would only do cymbalta before. But honestly nothing seems to work for fibro patients.

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
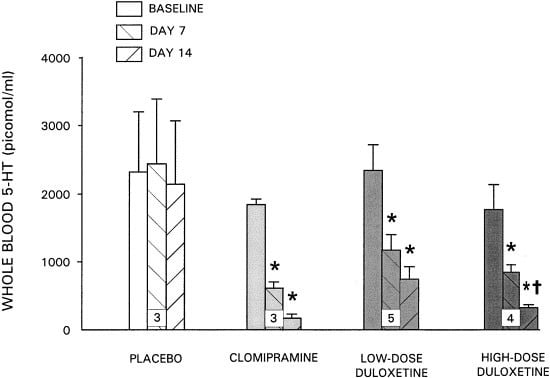
This is a comparison of relative, rather than absolute, effects. The fact of the matter is venlafaxine, desvenlafaxine, and duloxetine are weak NRIs, as shown by their inefficacy in blunting the tyramine pressor response (see below). I can't comment on milnacipran, because no such study has been conducted with it.Serotonin Norepinephrine Reuptake Inhibitors: A Pharmacological Comparison
The serotonin norepinephrine reuptake inhibitors are a family of antidepressants that inhibit the reuptake of both serotonin and norepinephrine. While these drugs are traditionally considered a group of inter-related antidepressants based upon reuptake ...

 www.nature.com
pubmed.ncbi.nlm.nih.gov
www.nature.com
pubmed.ncbi.nlm.nih.gov