
- Joined
- Apr 14, 2011
- Messages
- 178
- Reaction score
- 16
Hey guys
On the topic of nitrates
So FA2015 Page 305 notes that nitrates decrease preload >> afterload. When I think of nitrates, I think venodilation, whereas arteriolar dilation makes me think hydralazine.
Then I see this Uworld question where it makes me pick between the effects of nitrates: either only decreasing preload, or decreasing preload and after load the same amount.
Here's a snap of the two choices:
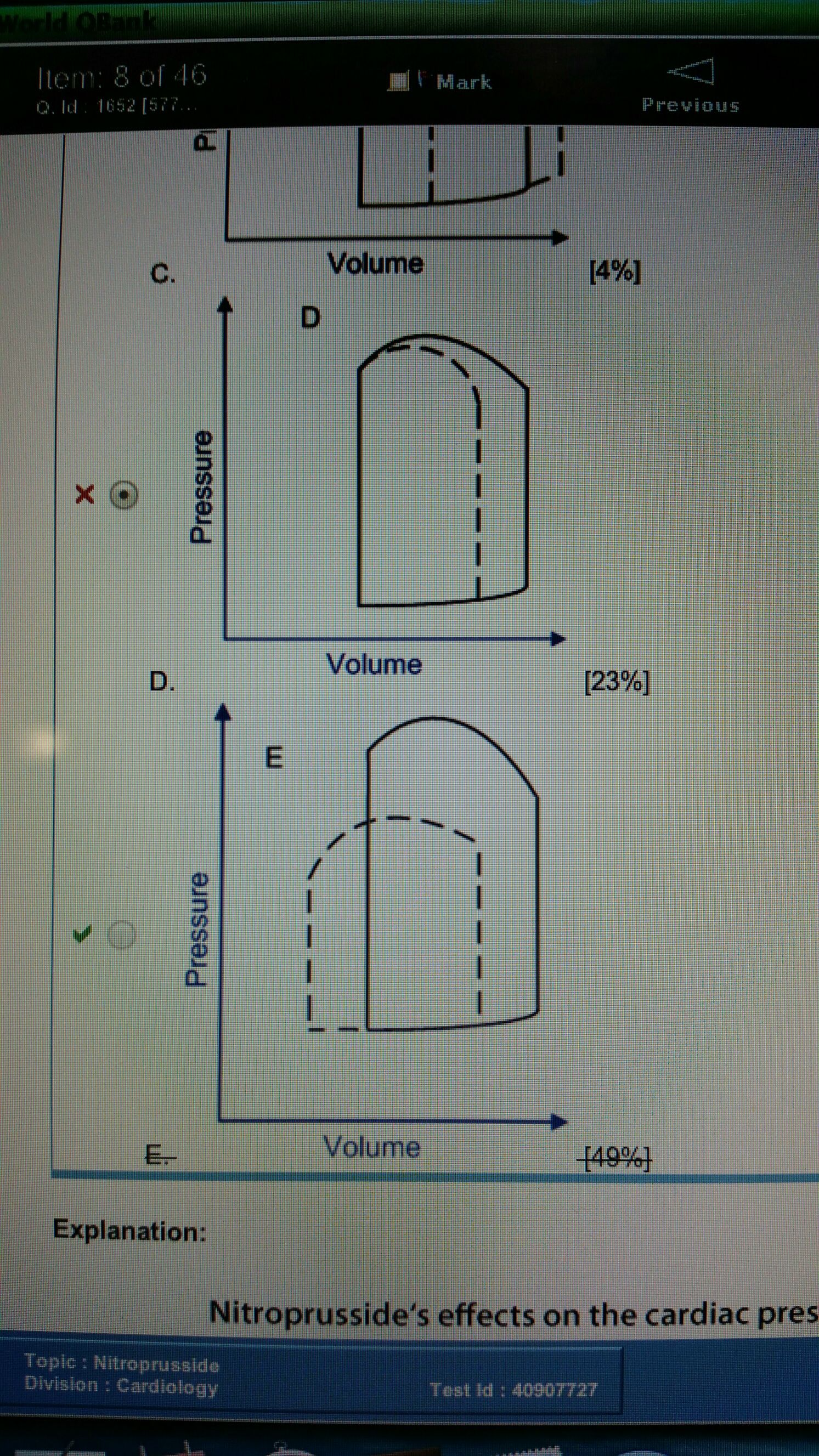
I'm concerned about picking the right one on test day, because this seems like a really important distinction.
Has anyone else had this mixup? What do you guys think?
Thanks in advance
On the topic of nitrates
So FA2015 Page 305 notes that nitrates decrease preload >> afterload. When I think of nitrates, I think venodilation, whereas arteriolar dilation makes me think hydralazine.
Then I see this Uworld question where it makes me pick between the effects of nitrates: either only decreasing preload, or decreasing preload and after load the same amount.
Here's a snap of the two choices:
I'm concerned about picking the right one on test day, because this seems like a really important distinction.
Has anyone else had this mixup? What do you guys think?
Thanks in advance