7
762513
We can, but the specific study you posted isn't an example of that.As I said, we all can play that game... of 'if' and/or cherry picking things

We can, but the specific study you posted isn't an example of that.As I said, we all can play that game... of 'if' and/or cherry picking things
Seriously, at what point during MS-III is one on par clinically with an NP? I'd say once someone has done 3-4 important cores, they're superior to an NP. Yet we have all these supervisory restrictions on 4th years/subIs (which is still for good reason).
Their values lie only in treating minor cases...Midlevels serve an important role. Any internist or subspecialist who has worked with NP/PAs know their great value. That doesn’t mean internists aren’t making a very big mistake by overly depending on consultants. IM can be making the same mistake anesthesiology made a couple decades ago.
It does not take a genius to figure out that a doctor with a specialty is better suited for certain conditions than a general practitioner. Of course, in their specialty they can do, most times, better than a doctor without that specific specialty. Still do not understand why that is even an issue... The issue here is that someone over here believes that NP's are better than MD's... ludicrous. The NP's can certainly treat minor situations or conditions. It is certainly impossible that they know as much as we do.
Glad you are proving our points... That's why they don't let 4th year med students practice medicine without supervision.... As for your second point: Well, it's a free country.I would take an experienced NP over an intern any day of the week. We can start discussing PGYII's tho if you would like...
No, their value is similar to that of an intern. They are educated eyes and ears who can spot when a doctor is needed and follow algorithms for preventative care.Their values lie only in treating minor cases...
Great opinion, drop some research findings that shows that.No, their value is similar to that of an intern. They are educated eyes and ears who can spot when a doctor is needed and follow algorithms for preventative care.
It's hard for me to argue with you if I don't know your credentials... Are you a doctor?No, their value is similar to that of an intern. They are educated eyes and ears who can spot when a doctor is needed and follow algorithms for preventative care.
Why would it be hard for you? Either his opinion has merit or it doesn't.It's hard for me to argue with you if I don't know your credentials... Are you a doctor?
Their knowledge doesn't even remotely come close to an interns. Like really, look at their curriculum. Unless the NP is spending all of their free time studying and reading medicine, how could they possible be as good?No, their value is similar to that of an intern. They are educated eyes and ears who can spot when a doctor is needed and follow algorithms for preventative care.
The experienced NP knows their daily routine via memorizing steps. They lack the breath and depth of knowledge to know when to include zebras into the differential & what to do for it. I'm sure some NPs spend their free time reading medicine and will know more, but how many do that for ongoing years?I would take an experienced NP over an intern any day of the week. We can start discussing PGYII's tho if you would like...
Yes I am. I supervise NP/PAs directly and work with subspecialists who employ them in clinics and in the hospital very well... As I plan to after I finish fellowship.It's hard for me to argue with you if I don't know your credentials... Are you a doctor?
By accountability I mean that these individuals do not take as much pharmacology, if any, or other courses that are mandatory in medical school, thus they do not possess the knowledge that may compare to what MD's know. This means that they are not held to the same standards as MD's, yet they are given the same responsibility?????
Not going to waste my time arguing with someone with no knowledge in healthcare about the utility of an intern vs. NP...Why would it be hard for you? Either his opinion has merit or it doesn't.
Their knowledge doesn't even remotely come close to an interns. Like really, look at their curriculum. Unless the NP is spending all of their free time studying and reading medicine, how could they possible be as good?
The experienced NP knows their daily routine via memorizing steps. They lack the breath and depth of knowledge to know when to include zebras into the differential & what to do for it. I'm sure some NPs spend their free time reading medicine and will know more, but how many do that for ongoing years?
Also I was comparing a fresh new NP vs. an MS-III 🙂
not really a proliferation of direct NP programs cuts out experience of bedside nursing .A fresh NP is still a nurse, and 95% of the time has had at least a few years at the bedside taking care of patients. I wouldn't go that far.
So you're saying that by being a nurse, they aren't capable of practicing medicine? Yet we give them independent rights 🙂A fresh NP is still a nurse, and 95% of the time has had at least a few years at the bedside taking care of patients. I wouldn't go that far.
Talking about arrogance when people with online degree and 500 hrs of preceptorship are claiming equivalency. Give me a break!Arrogance is why I prefer to work with midlevels over residents. NPs do their job at alerting the supervising doctor. Residents are too proud to say "I don't know".
not really a proliferation of direct NP programs cuts out experience of bedside nursing .
Shall we go into the list of things interns don't know but should? We can play this game all day. I'd take an NP over a PGY1, most people would. You're an outlier here.So you're saying that by being a nurse, they aren't capable of practicing medicine? Yet we give them independent rights 🙂
Being at the bedside taking care of patients means nothing when experienced RNs still don't know much about the various drugs they use or tests we order. How do I know that? Cause of the endless basic questions they ask.
How many doctors don't know what a lap chole is or what we use echos for? A ton of RNs don't know and some NPs (mind = blown) don't know either. The fact that even 1 exists is enough.
here is a list 6 pages long of programs that are direct to Masters. Im sure taking an convenience sample in your program is convenient , but is far from the reality out there.In my DNP program there are zero students without significant nursing experience. I'm on the low end with 5 years in critical care and 10 years in emergency medical services. I'm sure those exist, but I've never met an NP without significant bedside experience prior to becoming an NP. I feel 95% is a more than accurate number.
They aren't equal in knowledge. I have never seen an NP work entirely without at least the backup of an certified MD. You do not need a physician to ask a patient how they are doing with a ROS, do a physical exam, check routine labs, and recognize abnormalities for which they will notify promptly the supervising MD.Talking about arrogance when people with online degree and 500 hrs of preceptorship are claiming equivalency. Give me a break!
Do you think they should function independently as primary care without physicians backup or supervision , or in the roles you have listed?They aren't equal in knowledge. I have never seen an NP work entirely without at least the backup of an certified MD. You do not need a physician to ask a patient how they are doing with a ROS, do a physical exam, check routine labs, and recognize abnormalities for which they will notify promptly the supervising MD.
The bedside part to be honest is good, but does not contribute a lot in being a diagnostician... The way med students thing vs nurse is completely different. For instance, I am doing an ER rotation now and I am responsible to see 6+ patients a day, write my note, orders, present to my attending etc... in 7 hrs. When someone comes with a cough, I am already thinking about wide range of differentials by just looking at the patient's demographics. I did not think like that when I was a RN... Maybe I was a dumb RN.not really a proliferation of direct NP programs cuts out experience of bedside nursing .
Who would take a newer NP over a PGY1? The NP simply does not have the knowledge, period.Shall we go into the list of things interns don't know but should? We can play this game all day. I'd take an NP over a PGY1, most people would. You're an outlier here.
No I don't think they should be independent. But there is a very important role they serve and often they do a very good job at it from my experience.Do you think they should function independently as primary care without physicians backup or supervision , or in the roles you have listed?
Do you think they should function independently as primary care without physicians backup or supervision , or in the roles you have listed?
How do countries with few to no midlevels function then? They also do it cheaper.No I don't think they should be independent. But there is a very important role they serve and often they do a very good job at it from my experience.
This is a completely different argument... Still don't think they are safe. Primary care is too complicated to leave in the hands of experienced NP.I think there should be tiered NP independence program. A certain number of years with mandatory physician supervision, and then another board certification for independence. I think that would be a better standard than we have today. Do I think experienced NP's are safe in primary care? Yes.
When it comes to critical care, everyone I work with in the ICU, including the interns themselves, for starters. Are you still a medical student or are you in your residency?Who would take a newer NP over a PGY1? The NP simply does not have the knowledge, period.
They don't rely on subspecialists nearly to the extent that we do and there is not a threat of lawsuit nearly to the same extent. An internist or family med doc is treating a lot more than here and if they are wrong then be it. It is unfortunate that it is standard of care in this country to have specialists for simple cases. But since it is, midlevels can function just fine here under supervision.How do countries with few to no midlevels function then? They also do it cheaper.
The article splits treatment groups into younger healthier less co-morbid people vs older sicker people. What conclusion should we draw? That the NP group didn't harm the younger healthier subgroup? That the younger people, healther by study design, need an ED visit less?
What I'm curious about is what conclusions YOU are drawing from this.
I thought we weren't allowed to ask people for their credentials...When it comes to critical care, everyone I work with in the ICU, including the interns themselves, for starters. Are you still a medical student or are you in your residency?
In my DNP program there are zero students without significant nursing experience. I'm on the low end with 5 years in critical care and 10 years in emergency medical services. I'm sure those exist, but I've never met an NP without significant bedside experience prior to becoming an NP. I feel 95% is a more than accurate number.

Right, so the solution to liability is to allow nurses to diagnose and treat 🙂They don't rely on subspecialists nearly to the extent that we do and there is not a threat of lawsuit nearly to the same extent. An internist or family med doc is treating a lot more than here and if they are wrong then be it. It is unfortunate that it is standard of care in this country to have specialists for simple cases. But since it is, midlevels can function just fine here under supervision.
They don't rely on subspecialists nearly to the extent that we do and there is not a threat of lawsuit nearly to the same extent. An internist or family med doc is treating a lot more than here and if they are wrong then be it. It is unfortunate that it is standard of care in this country to have specialists for simple cases. But since it is, midlevels can function just fine here under supervision.
These are the docs that are destroying the profession for a few $$$....Pretty much the entire point. They're fine as extenders, helping with the low-acuity, moving the meat type of care. MLPs are fighting every single day for independent practice, and as you say you'll be emplying them after your fellowship, you'll essentially be "training" them to take that role. If MLPs keep advocating for independent practice, which they will, administration will see them as cheaper alternatives to you. Why bother with a fellow trained physician when they can hire an NP for much cheaper? They provide same care according to NP lobbyist.
Exactly. We have sell outs who want to kill the profession to get ahead a little it financially.These are the docs that are destroying the profession for a few $$$....
You literally just asked someone for their credentialsI thought we weren't allowed to ask people for their credentials...
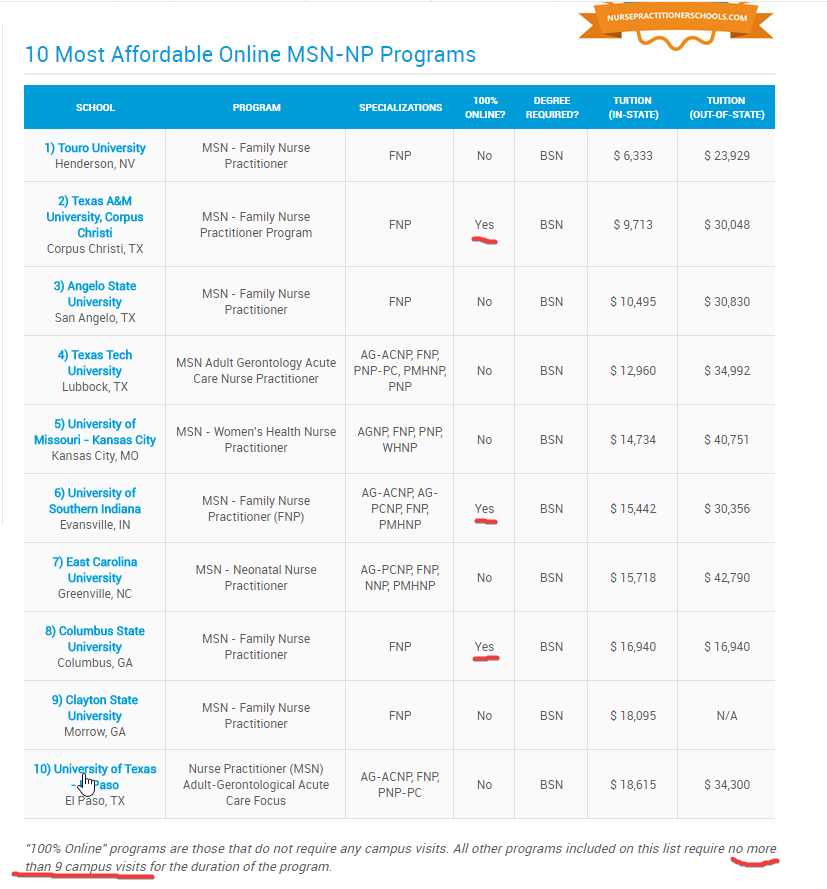
There's undoubtedly a problem with the inconsistent standards of NP programs. Here's 20 different MSN-NP/DNP programs where you only need to show up on campus NINE times throughout the entire program.
u
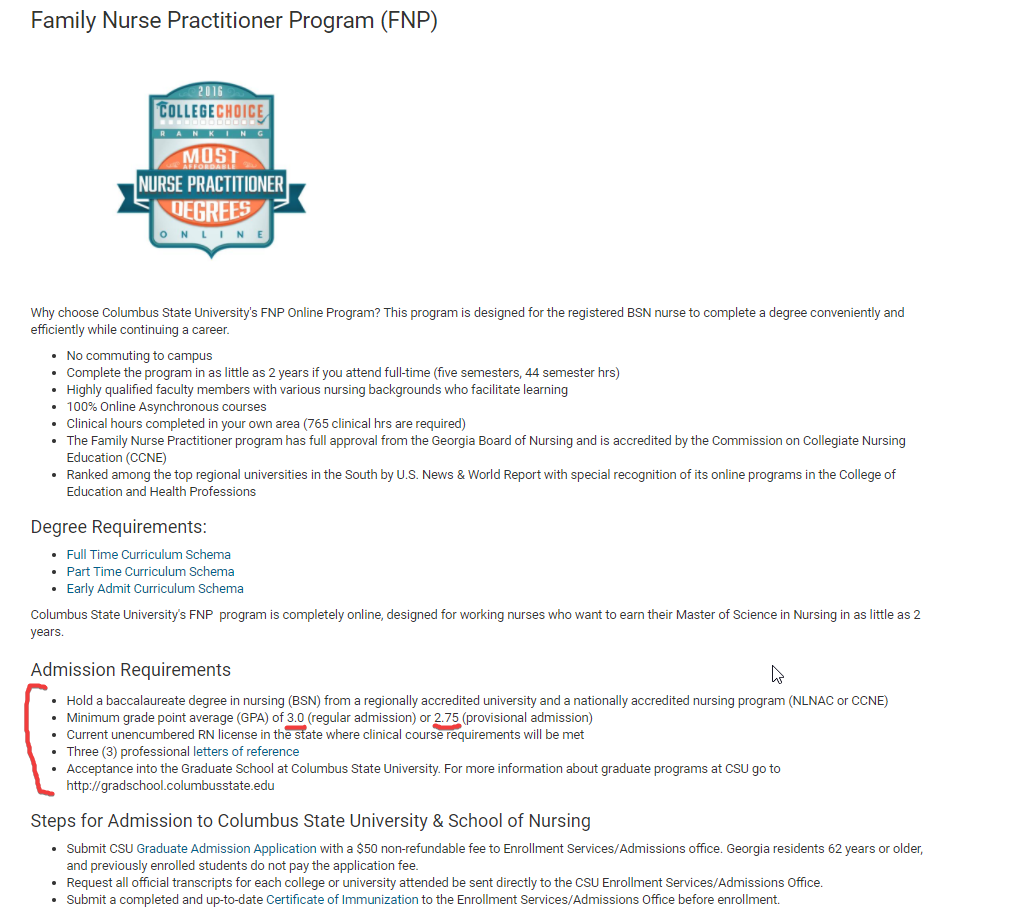
From Columbus State University FNP Online Program (100% online):
Family Nurse Practitioner Program
No mention of a requisite amount of clinical hours needed to get in, just a BSN and >2.75 GPA
So you have a non-zero amount of NPs who can get their BSN, get their DNP online, take a watered-down version of step 3 and then be able to hang up their shingle and try to claim "parity" with physicians.
They didn't include that finding in the conclusion because of the confounding variables you just listed. Don't call them out for concluding something that they actually didn't statistically conclude.
That's where it all starts. Then comes the pay cuts to you and allowing them to do more and more. Eventually you're supervising 5 NPs and see 10 patients a day yourself making half the money you used to.Reading some of these replies made me realize most people here have no real life experience. Go to almost any ED in the country and you'll see an NP working with the ED doc. Go to any community hospital and you will see NPs working with hospitalists. Go to any medicine or medical subspecialty clinic and you will see NPs monitoring patients with chronic medical conditions. Go to any surgery or surgical subspecialty clinic in the community and you will see an NP taking out stitches and asking how the patient is doing. This is not high-level diagnostic work. I don't want to spend more than a minute seeing a sickle cell patient coming in for pain medicine refill in a hematology clinic every few weeks. I don't want to see a stable chronic kidney disease patient in a nephrology patient without any change who just needs certain labs. The list goes on and on. NPs can do these roles "independently" but they are quick to notify the MD of any problem. In most countries these types of patients don't need subspecialists but in our country it is and hence we need NPs.
What do you mean? You realize med students do their clerkship in hospitals and doctors' office... We see these things you are sayingReading some of these replies made me realize most people here have no real life experience. Go to almost any ED in the country and you'll see an NP working with the ED doc. Go to any community hospital and you will see NPs working with hospitalists. Go to any medicine or medical subspecialty clinic and you will see NPs monitoring patients with chronic medical conditions. Go to any surgery or surgical subspecialty clinic in the community and you will see an NP taking out stitches and asking how the patient is doing. This is not high-level diagnostic work. I don't want to spend more than a minute seeing a sickle cell patient coming in for pain medicine refill in a hematology clinic every few weeks. I don't want to see a stable chronic kidney disease patient in a nephrology patient without any change who just needs certain labs. The list goes on and on. NPs can do these roles "independently" but they are quick to notify the MD of any problem. In most countries these types of patients don't need subspecialists but in our country it is and hence we need NPs.
But people here aren't saying they should be nonexistent, just that they should require supervision of a physicianReading some of these replies made me realize most people here have no real life experience. Go to almost any ED in the country and you'll see an NP working with the ED doc. Go to any community hospital and you will see NPs working with hospitalists. Go to any medicine or medical subspecialty clinic and you will see NPs monitoring patients with chronic medical conditions. Go to any surgery or surgical subspecialty clinic in the community and you will see an NP taking out stitches and asking how the patient is doing. This is not high-level diagnostic work. I don't want to spend more than a minute seeing a sickle cell patient coming in for pain medicine refill in a hematology clinic every few weeks. I don't want to see a stable chronic kidney disease patient in a nephrology patient without any change who just needs certain labs. The list goes on and on. NPs can do these roles "independently" but they are quick to notify the MD of any problem. In most countries these types of patients don't need subspecialists but in our country it is and hence we need NPs.