You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Osteopathic School Listed by MCAT Scores
- Thread starter ash118
- Start date

- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
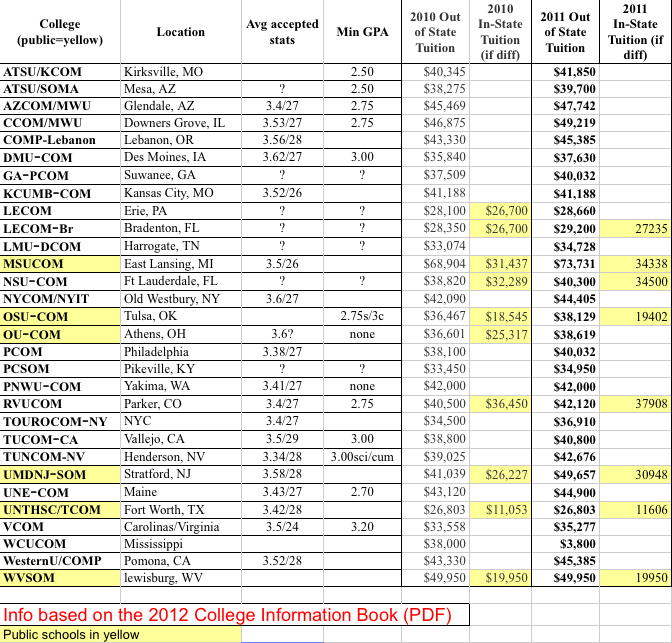
Unfortunately, a lot of this data is old, and in some cases, really old.
- Joined
- Mar 8, 2011
- Messages
- 1,673
- Reaction score
- 26
Compare my research vs the table and you can see it's pretty dated:
Rank by total MCAT numeric score
Osteopathic Medical School
Average MCAT scores**
(Bio, Phys, Essay, Verbal)
(Bio, Phys, Essay, Verbal)
1
10.00, 9.00, P, 9.00
Total= 28.00
2
9.01, 9.00, O, 8.76
Total= 26.77
Total= 26.77
3
9.01, 9.00, O, 8.76
Total= 26.77
Total= 26.77
4
Des Moines University College of Osteopathic Medicine, Des Moines, Iowa
9.35, 8.64, O, 8.65
Total= 26.64
Total= 26.64
5
University of North Texas Health Science Center Texas College of Osteopathic Medicine, Fort Worth, TX
9.20, 8.72, O, 8.49
Total= 26.41
Total= 26.41
6
Touro University College of Osteopathic Medicine, Vallejo, CA
9.07, 8.99, NR, 8.19
Total=26.25
Total=26.25
7
9.00, 8.00, O, 9.00
Total= 26.00
Total= 26.00
8
A.T. Still University of Health Sciences/Kirksville College of Osteopathic Medicine, Kirksville, MO
8.95, 8.25, O, 8.74
total= 25.94
total= 25.94
9
University of New England College of Osteopathic Medicine, Biddeford, Maine
8.80, 8.00, Q, 8.80
Total= 25.60
Total= 25.60
10
Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, FA
8.56, 8.00, O, 8.50
Total= 25.06
Total= 25.06
11
Michigan State University College of Osteopathic Medicine, East Lansing, MI
8.70, 8.00, O, 8.20
Total=24.90
Total=24.90
12
Kansas City University of Medicine and Biosciences, Kansas City, MO
8.64, 8.13, Q, 8.09
Total= 24.86
Total= 24.86
13
Philadelphia College of Osteopathic Medicine, Philadelphia, PA
8.56, 8.03, P, 8.08
Total= 24.67
Total= 24.67
14
Ohio University College of Osteopathic Medicine, Athens, OH
8.40, 7.55, P, 8.40
Total= 24.35
Total= 24.35
15
Edward Via Virginia College of Osteopathic Medicine, Blacksburg, VA
8.00, 8.00, P, 8.00
Total= 24.00
Total= 24.00
16
Lake Erie College of Osteopathic Medicine, Erie, PA
8.20, 7.60, O, 7.90
Total= 23.70
Total= 23.70
17
West Virginia School of Osteopathic Medicine, Lewisburg, WV
7.30, 6.80, N, 7.80
Total= 21.90
Total= 21.90
18
Pikeville College School of Osteopathic Medicine, Pikeville, KY
7.50, 6.90, O, 7.30
Total=21.70
Total=21.70
?
New York College of Osteopathic Medicine of New York Institute of Technology, Old Westbury, NY
Did NOT report
?
University of Medicine and Dentistry of New Jersey UMDNJ - School of Osteopathic Medicine, Strattford, NJ
Did NOT report
?
Lake Erie College of Osteopathic Medicine, Bradenton, FL campus
Did NOT report
?
Philadelphia College of Osteopathic Medicine Suwanee, GA campus
Did NOT report
?
Touro University Nevada College of Osteopathic Medicine, Henderson, NV campus
Did NOT report
?
Did NOT report
?
Did NOT report
?
Did NOT report
?
Did NOT report
?
Did NOT report
- Joined
- Aug 7, 2005
- Messages
- 4,947
- Reaction score
- 1,116
Very nice. Looks like DO schools are moving in stats and what worked a couple years ago isn't going to work in the near future.
- Joined
- May 26, 2010
- Messages
- 736
- Reaction score
- 39
IIRC they told us our incoming class (LECOM-E) was "almost" a 27 with a 3.45 cGPA
- Joined
- Aug 23, 2011
- Messages
- 1,941
- Reaction score
- 11
Great layout Danny. That should be pinned somewhere.
17West Virginia School of Osteopathic Medicine, Lewisburg, WV7.30, 6.80, N, 7.80
Total= 21.90
18Pikeville College School of Osteopathic Medicine, Pikeville, KY7.50, 6.90, O, 7.30
Total=21.70
?
This is sad. Are these the most up to date stats? If so, that's kinda pathetic.
- Joined
- Nov 30, 2010
- Messages
- 908
- Reaction score
- 13
This is sad. Are these the most up to date stats? If so, that's kinda pathetic.
Not sure if they are current; but bear in mind both of these campuses are several hours from civilization. Not a knock on the schools, just a point of fact.
Unfortunately, that by itself is going to drive down the stats as otherwise you can't get applicants. Doesn't mean anything about the education available, only that they chose to locate in rural mountainous regions that are applicant poor.
Unfortunately, that by itself is going to drive down the stats as otherwise you can't get applicants. Doesn't mean anything about the education available, only that they chose to locate in rural mountainous regions that are applicant poor.
While I agree with you, mostly, I still feel like these are very low standards for admission into medical school. It kinda makes me think about those people that claim that some DO schools are "degree mills". With a 21-22 MCAT average, I'm sure there are people getting in with high teen MCAT scores, which to me, is unacceptable for admission. Again, this just makes me doubt the credibility of the school and there supposed mission. I'm not necessarily saying that the education is any less, but the caliber of the admitted (average) student is less than any DO school or the Carib big 4.
I'm sure I'll get flamed for my opinion, but this is one of the reasons why I'm not applying to either of these schools. Do you even have to study to get a 20 MCAT?
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
Firstly, WVSOM's stat is really out of date, and it's closer to a 26 or 27 now, I believe. Secondly, Pikeville's stat is also out of date, but that school services and only accepts applicants from a very remote and limited region. Thus, less competition, and that's why it's so low.While I agree with you, mostly, I still feel like these are very low standards for admission into medical school. It kinda makes me think about those people that claim that some DO schools are "degree mills". With a 21-22 MCAT average, I'm sure there are people getting in with high teen MCAT scores, which to me, is unacceptable for admission. Again, this just makes me doubt the credibility of the school and there supposed mission. I'm not necessarily saying that the education is any less, but the caliber of the admitted (average) student is less than any DO school or the Carib big 4.
I'm sure I'll get flamed for my opinion, but this is one of the reasons why I'm not applying to either of these schools. Do you even have to study to get a 20 MCAT?
5University of North Texas Health Science Center Texas College of Osteopathic Medicine, Fort Worth, TX9.20, 8.72, O, 8.49
Total= 26.41
The above info is also dated... The TCOM website shows 28 for the last two years.
Firstly, WVSOM's stat is really out of date, and it's closer to a 26 or 27 now, I believe. Secondly, Pikeville's stat is also out of date, but that school services and only accepts applicants from a very remote and limited region. Thus, less competition, and that's why it's so low.
Well, this was my initial thought. And, after looking it up on their website, it is an average of 25 with an sGPA of 3.37. This is much more respectable and I retract what I said before. But, I stick with what I said about a 21 average MCAT being an ignoble admission standard. I'm glad to see a great improvement in these standards over the past few years.
- Joined
- Apr 28, 2010
- Messages
- 6,208
- Reaction score
- 36
I've also been concerned about this, but the truth is that Pikeville has indeed maintained rigor in accepting only a select number of applicants that meet their mission. Since that pool is incredibly small, I give them a "pass." WVSOM, on the other hand, needs to start bringing up those numbers. Unless the D.O. average hits 3.6/30, there will still be doubt as to how prepared D.O.'s are.Well, this was my initial thought. And, after looking it up on their website, it is an average of 25 with an sGPA of 3.37. This is much more respectable and I retract what I said before. But, I stick with what I said about a 21 average MCAT being an ignoble admission standard. I'm glad to see a great improvement in these standards over the past few years.
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
Let me get accepted first, before we start talking about needlessly raising stats simply for the sake of appearance.I've also been concerned about this, but the truth is that Pikeville has indeed maintained rigor in accepting only a select number of applicants that meet their mission. Since that pool is incredibly small, I give them a "pass." WVSOM, on the other hand, needs to start bringing up those numbers. Unless the D.O. average hits 3.6/30, there will still be doubt as to how prepared D.O.'s are.
Let me get accepted first, before we start talking about needlessly raising stats simply for the sake of appearance.
For the sake of appearance? That's not really the point. Also, it's not a "needless" act either. I think this is something that should be done over time.
Like I said, a 25 is fine for now. But, within the next decade, I hope this score rises to ~28. I'm not hoping for anything radical.
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
You do realize that at one point, the average MD MCAT score was under a 30 too, right? And the average accepted DO MCAT these days is almost a 27.For the sake of appearance? That's not really the point. Also, it's not a "needless" act either. I think this is something that should be done over time.
Like I said, a 25 is fine for now. But, within the next decade, I hope this score rises to ~28. I'm not hoping for anything radical.
You guys should stop worrying about what people's average MCAT scores are. Your medical school curriculum, clinical rotations, and residency are much more important. By the time you graduate from your residency, your MCAT score will be at least eight years old. It's not that important.
You do realize that at one point, the average MD MCAT score was under a 30 too, right? And the average accepted DO MCAT these days is almost a 27.
You guys should stop worrying about what people's average MCAT scores are. Your medical school curriculum, clinical rotations, and residency are much more important. By the time you graduate from your residency, your MCAT score will be at least eight years old. It's not that important.
Once you start medical school, MCAT scores are about as relevant as your 7th grade marks
- Joined
- Jul 17, 2008
- Messages
- 608
- Reaction score
- 9
Definitely not, and I think those 21 averages are WAY out of date.I'm sure I'll get flamed for my opinion, but this is one of the reasons why I'm not applying to either of these schools. Do you even have to study to get a 20 MCAT?
- Joined
- Jun 30, 2011
- Messages
- 534
- Reaction score
- 0
definitely agree with this! I might be premed but my dad is a top doctor at his hospital and works with 3rd years of both MD and DOs....and he frankly is always more impressed with DOs and he tells me its because many DOs are older and have more life experience and seem more prepared. Also when I speak with new residents most dont even remember their MCAT....and as the avg scores for MD schools go up so will the avg scores for DO schools and just because an applicant has a lower score doesn't mean they will be a stupid doctor. you really shouldnt compare mcat scores to compare schools because your not on the admissions committee and have no clue what they are using to admit people especially with DO schools who truly strive to look at a person holistically unlike many MD schools.Once you start medical school, MCAT scores are about as relevant as your 7th grade marks
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
Exactly right. At my age, if I worried about my scores were eight years ago, I would be talking about elementary school, lol.Once you start medical school, MCAT scores are about as relevant as your 7th grade marks
- Joined
- Aug 16, 2007
- Messages
- 273
- Reaction score
- 7
I know two doctors who are still practicing and they are both in their early seventies. They informed me that when they applied to medical school, they didn't even 'study' for the MCAT. From what one of them said, the MCAT didn't even release his score to him until he applied to school. He applied to TWO schools and got into both.
He was shocked when I told him that I studied for at least 250 hours for my test and that I am applying to 20 schools!
He was shocked when I told him that I studied for at least 250 hours for my test and that I am applying to 20 schools!
- Joined
- Mar 19, 2006
- Messages
- 3,015
- Reaction score
- 11
This is the same list I saw when I first started thinking to applying to DO schools 5 years ago... and it was out of date THEN.
Also, on another note, someone mentioned that it is unacceptable to accept anyone with MCAT in the teens. My question to you pre-meds is: why? The MCAT is just a standardized test, it gives you no information on whether or not that person will become a good physician. I would actually argue that its a bell curve with the most average MCATs probably becoming the best physicians. And this is coming from someone who did well on the MCAT (32)
Also, on another note, someone mentioned that it is unacceptable to accept anyone with MCAT in the teens. My question to you pre-meds is: why? The MCAT is just a standardized test, it gives you no information on whether or not that person will become a good physician. I would actually argue that its a bell curve with the most average MCATs probably becoming the best physicians. And this is coming from someone who did well on the MCAT (32)
- Joined
- Jun 30, 2011
- Messages
- 534
- Reaction score
- 0
I don't have a source for his info but my TA in my histology class told me that they did studies on the MCAT and determined that the PS and BS were good indicators on how well you perform in med school and VR was a good indicator on how well of a physician you will be. this isn't my opinion was just told by my TAThis is the same list I saw when I first started thinking to applying to DO schools 5 years ago... and it was out of date THEN.
Also, on another note, someone mentioned that it is unacceptable to accept anyone with MCAT in the teens. My question to you pre-meds is: why? The MCAT is just a standardized test, it gives you no information on whether or not that person will become a good physician. I would actually argue that its a bell curve with the most average MCATs probably becoming the best physicians. And this is coming from someone who did well on the MCAT (32)
- Joined
- Mar 19, 2006
- Messages
- 3,015
- Reaction score
- 11
I don't have a source for his info but my TA in my histology class told me that they did studies on the MCAT and determined that the PS and BS were good indicators on how well you perform in med school and VR was a good indicator on how well of a physician you will be. this isn't my opinion was just told by my TA
I know the studies you are referring to. VR good indicator of board scores is the conclusion.. Again, how does that translate into becoming a competent physician? Medical knowledge is 50% or less of that in my humble opinion.
- Joined
- Apr 28, 2010
- Messages
- 6,208
- Reaction score
- 36
Yes, they were, but do you realize that today's applicant and doctors are much better than those back then? MCAT scores have been correlated to better performance in the USMLE. Better performance in the USMLE means better chances at a better residency. Better residency means better fellowships and job opportunities, which means that the representation of D.O.'s in the upper echelon increases and helps the entire profession.You do realize that at one point, the average MD MCAT score was under a 30 too, right? And the average accepted DO MCAT these days is almost a 27.
You guys should stop worrying about what people's average MCAT scores are. Your medical school curriculum, clinical rotations, and residency are much more important. By the time you graduate from your residency, your MCAT score will be at least eight years old. It's not that important.
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
You think today's doctors are better than those who came before them? Say even a few years before them? The reason why MCAT scores are higher is due to increased availability to prep material, not because they're "better". I would take a doctor who has been in the profession for twenty years over one who just graduated. And I keep telling you that it's all relative. If the average accepted DO MCAT score reaches a 30, then that means that MD MCAT scores are around 33 or 34. That's just how it's been. BTW, better USMLE scores don't necessarily mean better residencies, not if the competition is getting harsher, which once again is due to better test prep material.Yes, they were, but do you realize that today's applicant and doctors are much better than those back then? MCAT scores have been correlated to better performance in the USMLE. Better performance in the USMLE means better chances at a better residency. Better residency means better fellowships and job opportunities, which means that the representation of D.O.'s in the upper echelon increases and helps the entire profession.
It's all relative. BTW, you really shouldn't be caring about how DO's are perceived. When you start working, you'll realize that no one really cares if you're a DO or MD.
EDIT: BTW, DO schools can't just only start accepting applicants with MCAT scores above a 30. Those guys will probably also get accepted into an MD school, and will likely choose an MD school over a DO one. To change that, DO schools have to improve their curriculum, connections, and rotation sites (all while lowering tuition), so as to attract these higher scored candidates. Until that day, the only way the DO average will be a 30, is if a 30 just isn't good enough to get into MD schools anymore.
- Joined
- Mar 19, 2006
- Messages
- 3,015
- Reaction score
- 11
You think today's doctors are better than those who came before them? Say even a few years before them? The reason why MCAT scores are higher is due to increased availability to prep material, not because they're "better". I would take a doctor who has been in the profession for twenty years over one who just graduated. And I keep telling you that it's all relative. If the average accepted DO MCAT score reaches a 30, then that means that MD MCAT scores are around 33 or 34. That's just how it's been. BTW, better USMLE scores don't necessarily mean better residencies, not if the competition is getting harsher, which once again is due to better test prep material.
It's all relative. BTW, you really shouldn't be caring about how DO's are perceived. When you start working, you'll realize that no one really cares if you're a DO or MD.
EDIT: BTW, DO schools can't just only start accepting applicants with MCAT scores above a 30. Those guys will probably also get accepted into an MD school, and will likely choose an MD school over a DO one. To change that, DO schools have to improve their curriculum, connections, and rotation sites (all while lowering tuition), so as to attract these higher scored candidates. Until that day, the only way the DO average will be a 30, is if a 30 just isn't good enough to get into MD schools anymore.
Actually, a recent large study concluded younger docs have better outcomes than older more experienced docs..
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
Don't care. Younger docs are only good due to the knowledge they're being taught by older docs. That's the whole point really of residency. Either way, the rest of my point still stands.Actually, a recent large study concluded younger docs have better outcomes than older more experienced docs..
- Joined
- Mar 19, 2006
- Messages
- 3,015
- Reaction score
- 11
Don't care. Younger docs are only good due to the knowledge they're being taught by older docs. That's the whole point really of residency. Either way, the rest of my point still stands.
Edit- Two studies:
http://www.annals.org/content/142/4/I-54.full
http://www.amjmed.com/article/S0002-9343(11)00319-6/abstract
- Joined
- Mar 19, 2006
- Messages
- 3,015
- Reaction score
- 11
Don't care. Younger docs are only good due to the knowledge they're being taught by older docs. That's the whole point really of residency. Either way, the rest of my point still stands.
😕😕😕 You're saying if they are better, it's because of the knowledge gained from previous generations. To that I say: Of course! That's pretty common sense, right? But how they got better doesn't change the argument that they are better.
Edit: In case anyone actually reads the studies I referenced, they are flawed, but I think younger docs really are better at many aspects of healthcare. Not all aspects, though.
Last edited:
- Joined
- Apr 28, 2006
- Messages
- 6,133
- Reaction score
- 2,369
I know the studies you are referring to. VR good indicator of board scores is the conclusion.. Again, how does that translate into becoming a competent physician? Medical knowledge is 50% or less of that in my humble opinion.
So you're saying that medical knowledge is less than 50% of what determines competence? Really?
Honestly, if you can't break a 20 on the MCAT you probably shouldn't be a doctor
- Joined
- Mar 19, 2006
- Messages
- 3,015
- Reaction score
- 11
So you're saying that medical knowledge is less than 50% of what determines competence? Really?
Honestly, if you can't break a 20 on the MCAT you probably shouldn't be a doctor
Maybe exaggerated, but I stand behind the point - much more to medicine than textbook knowledge.
I still don't see why 10 or 20 or 30 is a magic cutoff.. Its a standardized test.. im not sure it actually tests anything other than how well you can take a test.
My question to you pre-meds is: why? The MCAT is just a standardized test, it gives you no information on whether or not that person will become a good physician.
That was me and I feel like Triage summed it up pretty well:
MCAT scores have been correlated to better performance in the USMLE. Better performance in the USMLE means better chances at a better residency. Better residency means better fellowships and job opportunities, which means that the representation of D.O.'s in the upper echelon increases and helps the entire profession.
While the correlation between the MCAT and USMLE (not sure about COMLEX) isn't that strong, it is still a decent indicator. For all intents and purposes (meaning there is a correlation, albeit imperfect), a better MCAT means a better USMLE score leading to better residency/fellowship opportunities. This leads to better training and theoretically a better physician. Please realize that this is a generalization and there will always be some exceptions.
Also, I think a high teen score on the MCAT indicates a fundamental lack of basic science principles, critical thinking, and application of knowledge: all core characteristics of a good physician IMO. It's not "just a test".
Additionally, you really don't have to study to get a score this low. This makes me doubt the individual's motivation and passion to succeed.
Honestly, if you can't break a 20 on the MCAT you probably shouldn't be a doctor
Totally agree.
EDIT: BTW, DO schools can't just only start accepting applicants with MCAT scores above a 30.
They do accept applicants with above a 30 and some matriculate 😕
- Joined
- May 31, 2011
- Messages
- 315
- Reaction score
- 2
You think today's doctors are better than those who came before them? Say even a few years before them? The reason why MCAT scores are higher is due to increased availability to prep material, not because they're "better". I would take a doctor who has been in the profession for twenty years over one who just graduated. And I keep telling you that it's all relative. If the average accepted DO MCAT score reaches a 30, then that means that MD MCAT scores are around 33 or 34. That's just how it's been. BTW, better USMLE scores don't necessarily mean better residencies, not if the competition is getting harsher, which once again is due to better test prep material.
It's all relative. BTW, you really shouldn't be caring about how DO's are perceived. When you start working, you'll realize that no one really cares if you're a DO or MD.
EDIT: BTW, DO schools can't just only start accepting applicants with MCAT scores above a 30. Those guys will probably also get accepted into an MD school, and will likely choose an MD school over a DO one. To change that, DO schools have to improve their curriculum, connections, and rotation sites (all while lowering tuition), so as to attract these higher scored candidates. Until that day, the only way the DO average will be a 30, is if a 30 just isn't good enough to get into MD schools anymore.
I would most certainly disagree with you.
1) I definitely think the newer doctors will be better than the older doctors. Newer doctors are aware of newer drugs, newer treatments, and are trained in newer techniques. For example, I shadowed a youngish (late 40s) orthopedic surgeon who was trying out a new, experimental procedure. It involved centrifugation, construction of a new femur head, and stem cell therapy, all in the OR. He was working as part of a surgical team with an older doc. The older doc was not comfortable performing the procedure as he was less familiar with the techniques.
Obviously, this does not prove the case that younger docs > older docs. But I think it's a snapshot of what should be pretty obvious. The older you get, the less willing you are to change your style and learn new things. It's why the average "younger" person is so much better with computers and technology than the average "older" person. I'm clearly using generalities here, but you understand what I'm saying. The average med school matriculant is smarter (fiercer and more competition than ever before means only the smartest make it through), has to learn more (increased volume of medical knowledge with each year), and has a greater dearth of technology and tools to use.
I believe this applies all across the board, actually. Quantum physicists are more intelligent than ever before, Engineers are more creative and complex, and Doctors have more tools, giving them the opportunity to perform better. Increased intelligence means increased technology/knowledge, means increased effectiveness. At least, that's how I perceive it. Please feel free to refute me, I'd love to read your response (no sarcasm at all).
2) I have an MCAT>30, and I would rather go to a DO school than an MD school. Granted, this wasn't my opinion before I started out this process. But researching osteopathy, shadowing 2 DOs (i've shadowed 6 MDs), and speaking with osteopathic vs. allopathic admissions offices completely changed my opinion. I may not get in this cycle - and I could definitely better myself as an applicant to be competitive at MD by next year. But I'm tailoring all of my efforts to go to a DO school because I would love to be ksmajmudar, DO.
Last edited:
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
OK, fine. Younger docs= better docs. That's not really my point, though. You may have chosen DO over MD, but you're the exception to the norm. Personally, I understand why many would choose DO over MD, as I also prefer the philosophy of it. Unfortunately, most choose MD, and that's why the MD accepted stats (overall) are always higher than DO average stats.I would most certainly disagree with you.
1) I definitely think the newer doctors will be better than the older doctors. Newer doctors are aware of newer drugs, newer treatments, and are trained in newer techniques. For example, I shadowed a youngish (late 40s) orthopedic surgeon who was trying out a new, experimental procedure. It involved centrifugation, construction of a new femur head, and stem cell therapy, all in the OR. He was working as part of a surgical team with an older doc. The older doc was not comfortable performing the procedure as he was less familiar with the techniques.
Obviously, this does not prove the case that younger docs > older docs. But I think it's a snapshot of what should be pretty obvious. The older you get, the less willing you are to change your style and learn new things. It's why the average "younger" person is so much better with computers and technology than the average "older" person. I'm clearly using generalities here, but you understand what I'm saying. The average med school matriculant is smarter (fiercer and more competition than ever before means only the smartest make it through), has to learn more (increased volume of medical knowledge with each year), and has a greater dearth of technology and tools to use.
I believe this applies all across the board, actually. Quantum physicists are more intelligent than ever before, Engineers are more creative and complex, and Doctors have more tools, giving them the opportunity to perform better. Increased intelligence means increased technology/knowledge, means increased effectiveness. At least, that's how I perceive it. Please feel free to refute me, I'd love to read your response (no sarcasm at all).
2) I have an MCAT>30, and I would rather go to a DO school rather than an MD school. Granted, this wasn't my opinion before I started out this process. But researching osteopathy, shadowing 2 DOs (i've shadowed 6 MDs), and speaking with osteopathic vs. allopathic admissions offices completely changed my opinion. I may not get in this cycle - and I could definitely better myself as an applicant to be competitive at MD by next year. But I'm tailoring all of my efforts to go to a DO school because I would love to be ksmajmudar, DO.
If DO accepted stats reach a 30 average MCAT, then that means that MD average stats are 33 or 34. It's just the way it is. That doesn't mean that DO's are any worse, though. DO's can be as good as anyone else.
I would argue, though, that public perception of DO's will always be of ignorance. Why? Because 80% of medical graduates are MD's. That's why. The reason why the public doesn't know much about DO's isn't because DO's don't get into ROAD specialties, it's because the vast majority of doctors that patients encounter are MD's.
- Joined
- Jun 30, 2011
- Messages
- 534
- Reaction score
- 0
I have to disagree about the competitive nature as many med schools r pushing for pass/fail instead of grades to reduce competition so students are getting less competitive then years before
- Joined
- Feb 24, 2005
- Messages
- 15,463
- Reaction score
- 1,908
I think it would be pretty easy to base any cutoffs around the mean of 25. You should be able to get in the top half on the test given the test taking population.Maybe exaggerated, but I stand behind the point - much more to medicine than textbook knowledge.
I still don't see why 10 or 20 or 30 is a magic cutoff.. Its a standardized test.. im not sure it actually tests anything other than how well you can take a test.
If DO accepted stats reach a 30 average MCAT, then that means that MD average stats are 33 or 34. It's just the way it is. That doesn't mean that DO's are any worse, though. DO's can be as good as anyone else.
No, that's not the "way it is". The admissions standards for DO schools will not ever necessarily equal the admissions standards for MD schools, but I do believe the gap will become more narrow. As for the average MCAT, it is going to level off eventually. If the average MCAT for MD schools was 33-34, there wouldn't be many applicants. Less applicants, less matriculants, less working physicians which contradicts the mission of many medical schools.
Plus, that means more people would apply to DO schools, which means there would be more DO's pumped into the population to work. Coincidentally, this counters your next point.
I would argue, though, that public perception of DO's will always be of ignorance. Why? Because 80% of medical graduates are MD's. That's why. The reason why the public doesn't know much about DO's isn't because DO's don't get into ROAD specialties, it's because the vast majority of doctors that patients encounter are MD's.
I agree with the point, but with more DO schools being built, there are obviously going to be more DO's practing throughout the US. Again, the gap is going to narrow (although it may never be equal).
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
You can build as many DO schools as you want, and have plenty of people applying to DO schools. If the number of residencies don't increase, then who cares? BTW, new MD schools are also being built.No, that's not the "way it is". The admissions standards for DO schools will not ever necessarily equal the admissions standards for MD schools, but I do believe the gap will become more narrow. As for the average MCAT, it is going to level off eventually. If the average MCAT for MD schools was 33-34, there wouldn't be many applicants. Less applicants, less matriculants, less working physicians which contradicts the mission of many medical schools.
Plus, that means more people would apply to DO schools, which means there would be more DO's pumped into the population to work. Coincidentally, this counters your next point.
I agree with the point, but with more DO schools being built, there are obviously going to be more DO's practing throughout the US. Again, the gap is going to narrow (although it may never be equal).
If you want to make the public more aware of DO's, then more effort needs to be put into OGME residencies (along with the new DO schools), and have those residencies be in diverse specialties.
- Joined
- Mar 19, 2006
- Messages
- 3,015
- Reaction score
- 11
While the correlation between the MCAT and USMLE (not sure about COMLEX) isn't that strong, it is still a decent indicator. .
No physician would use a medical test with the sensitivity and specificity of the MCAT.
- Joined
- Apr 28, 2010
- Messages
- 6,208
- Reaction score
- 36
Aside from Kuba's point, you're basically saying that if given the option between using floppy disks now and have blue rays in 20 years, you prefer using floppy disks now and continue using them 20 years later. You make no sense.Don't care. Younger docs are only good due to the knowledge they're being taught by older docs. That's the whole point really of residency. Either way, the rest of my point still stands.
- Joined
- Aug 28, 2009
- Messages
- 1,682
- Reaction score
- 12
What? Are you saying that newer docs have the capability to somehow hold more data?Aside from Kuba's point, you're basically saying that if given the option between using floppy disks now and have blue rays in 20 years, you prefer using floppy disks now and continue using them 20 years later. You make no sense.
- Joined
- Nov 10, 2009
- Messages
- 16,447
- Reaction score
- 8,630
What? Are you saying that newer docs have the capability to somehow hold more data?
Sigh... you're diluted...
A doctor who received his educated 10 years ago will inevitably know less than a doctor who received his educated today. Why? Because technology and research based procedures have been invented or changed during that time, and while the older doctor has learned to use the newer stuff, the newer doctor only knows how to use the newer tech and in more depth.
It's like asking a 8 year old to learn to use the computer for the first time as opposed to a 40 year old. In majority the 8 year olds will learn to use it as if it was an extension of their own bodies.
Either way this debate is incredibly pointless and moot.
- Joined
- Nov 10, 2009
- Messages
- 16,447
- Reaction score
- 8,630
No physician would use a medical test with the sensitivity and specificity of the MCAT.
Psychiatrists do... all the time lol.
- Joined
- Jul 23, 2008
- Messages
- 2,922
- Reaction score
- 1,517
So you're saying that medical knowledge is less than 50% of what determines competence? Really?
Honestly, if you can't break a 20 on the MCAT you probably shouldn't be a doctor
Seriously. I understand the whole "holistic" approach to applicants, but cmon. <20 is just ridiculous, that means you scored in <40th percentile in every section.
- Joined
- Apr 25, 2011
- Messages
- 75
- Reaction score
- 0
Sigh... you're diluted...
A doctor who received his educated 10 years ago will inevitably know less than a doctor who received his educated today. Why? Because technology and research based procedures have been invented or changed during that time, and while the older doctor has learned to use the newer stuff, the newer doctor only knows how to use the newer tech and in more depth.
It's like asking a 8 year old to learn to use the computer for the first time as opposed to a 40 year old. In majority the 8 year olds will learn to use it as if it was an extension of their own bodies.
Either way this debate is incredibly pointless and moot.
Paragraph 1: Huh?
Paragraph 2: 👍
IMO, MCAT = Level of first restart on Angry Birds.
- Joined
- Nov 10, 2009
- Messages
- 16,447
- Reaction score
- 8,630
Seriously. I understand the whole "holistic" approach to applicants, but cmon. <20 is just ridiculous, that means you scored in <40th percentile in every section.
Well when your mean applicant score for schools like Pikesvile or WVSOM is extremely low, you're inevitably going to have to fill a seat with a very low stat student.
- Joined
- Nov 10, 2009
- Messages
- 16,447
- Reaction score
- 8,630
Paragraph 1: Huh?
Paragraph 2: 👍
IMO, MCAT = Level of first restart on Angry Birds.
Yah... the first paragraph is a bit rough... Basically I just mean that the newer doctor learned newer more efficient methods his first time around as opposed to the older doctor, who had to learn it on top of the older procedures which are now obsolete.
Similar threads
- Replies
- 0
- Views
- 10K