I'm doing this rough and dirty remotely. A H&N patient, don't have an MRI, so just put in "spheres" as hippocamp surrogates because too lazy to tease them out right now. So this is just a planning study/example. Put 0.5cm around those (spheres-marg). Subtract from normal brain (brain-minus). Lens-L is actually both lenses. Contoured in lenses, and parotids, but note I did not have to place any constraints on them due to beam placement. Arcs don't present/aim all optimal vectors on things (ie eyes, throat, lenses, parotids) we mean to miss; they never do but this is real evident in WBRT. This beam arrangement would show the optimal vectors if we could move couch and gantry at same time for an arc. Of course can't do that, so therefore here we are with static beams. Meant to put on 9 beams but lost count and put on 10.
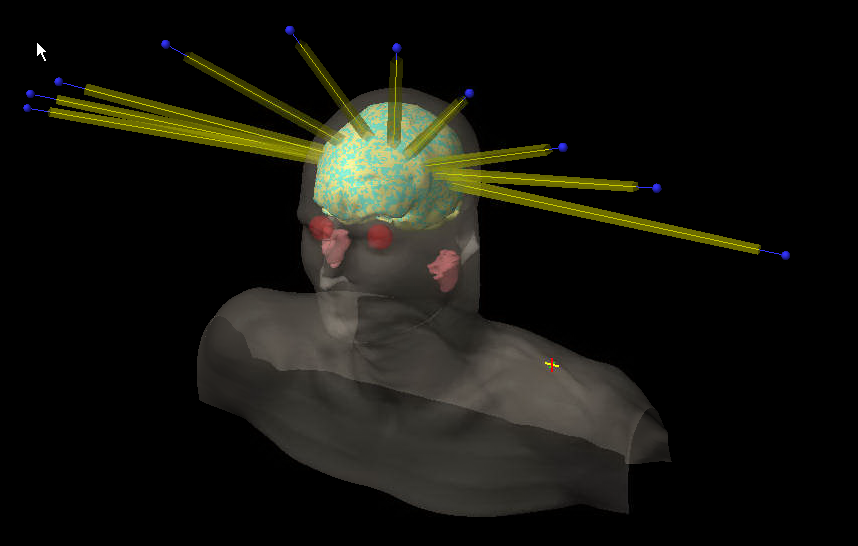
A 9 field approach with beams like this:
optimized like this:
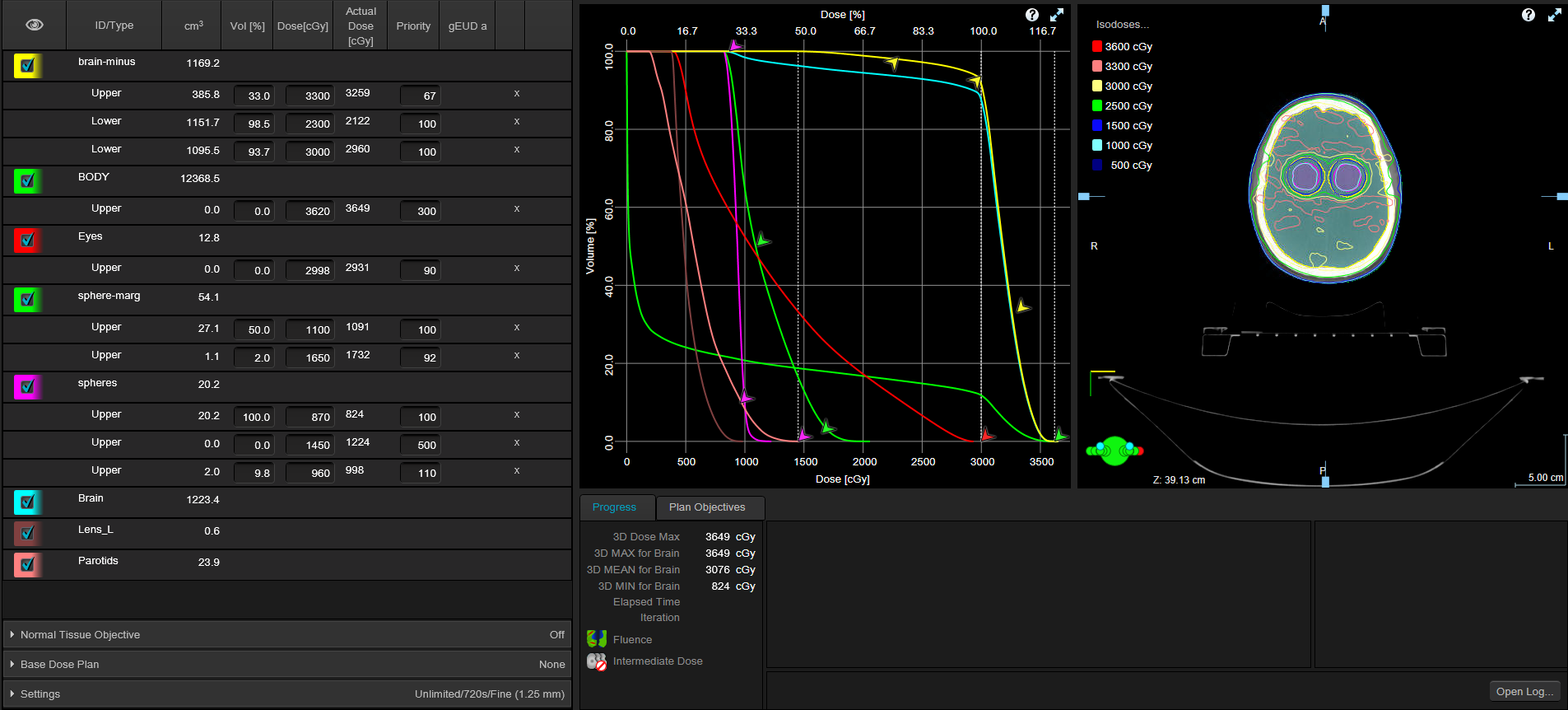
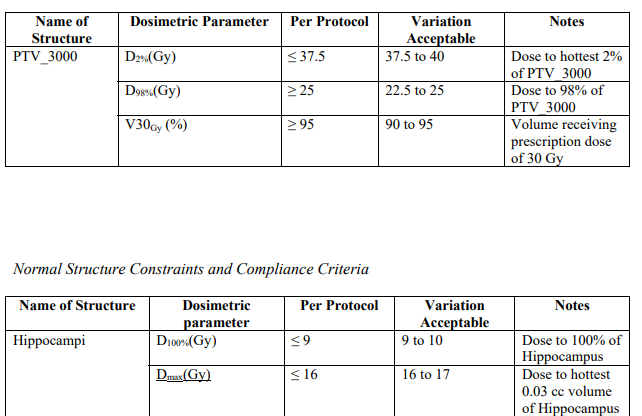
Paying attention to constraints like this:
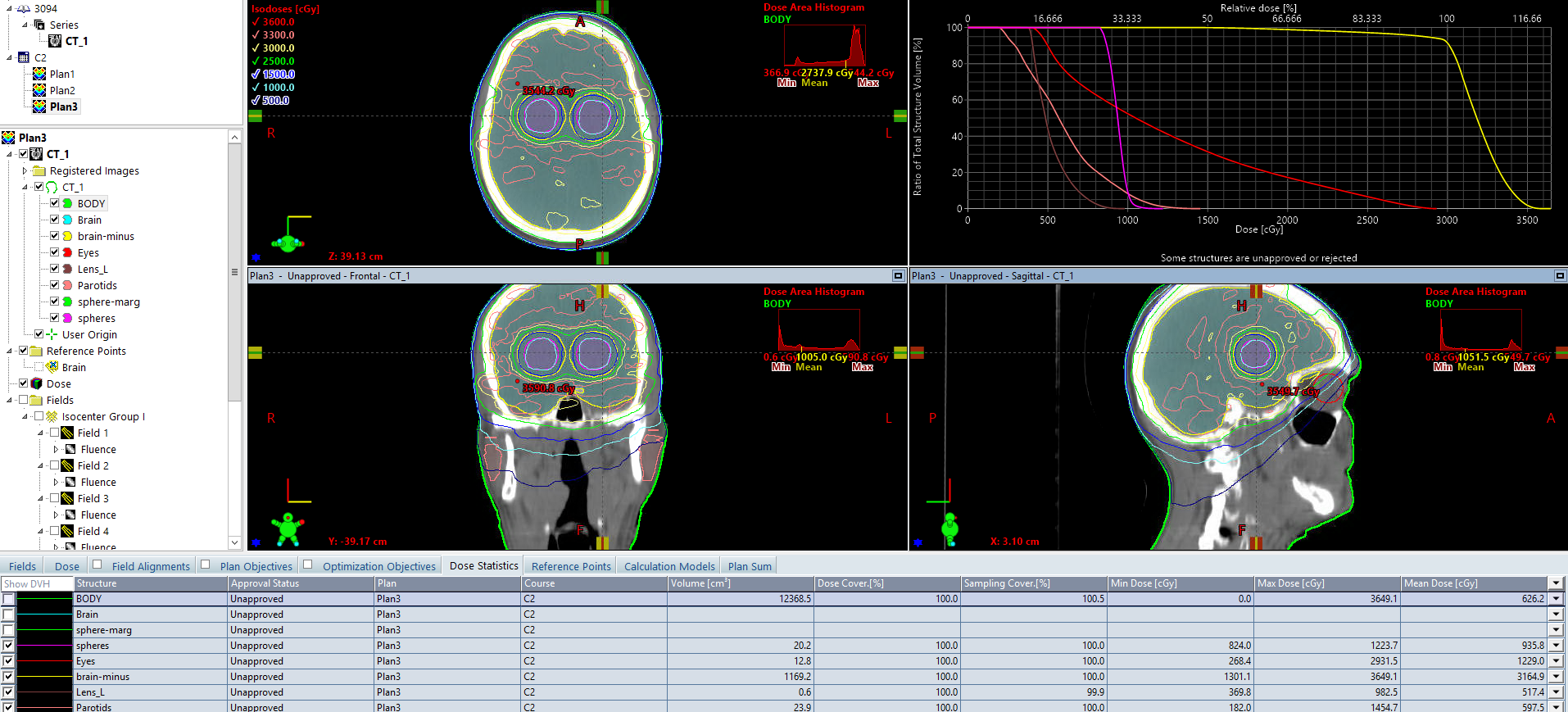
And get dose distributions/DVH like this:
This was all planned and calc'd in ~30 min. Parotids maxing at ~15 Gy and lenses at ~10 Gy with zero effort. Only about 1/3 normal brain above 110% dose. The beams are about 300 MUs per beam which will take ~30 seconds per beam to deliver at 600 MU/min dose rate; at 10 beams, we're talking ~300 second total beam on time. Of course must kick couch and rotate gantry between beams so tx time will be much longer but very doable. There is no way (I think) to get eye sparing (or parotid sparing?) like this with arcs IMHO.
And I can get the seahorse lower than commonly shown/reported. YMMV.