
- Joined
- Feb 25, 2010
- Messages
- 4,263
- Reaction score
- 1,560
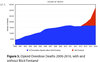
Prescription ODs have leveled off, while illicit fentanyl ODs are skyrocketing, but the media is lumping them all in one big basket called the ‘opiate crisis,’ not making the important distinction. The illicit drug markets have nothing to do with doctors, pharmacies or pharmaceutical companies at all. I’m not saying that we in the medical community shouldn’t look for ways to improve things. We should. But we could prescribe zero opiates next year and the skyrocketing illicit fentanyl ODs won’t be affected one bit. Everyone lumps the two separate problems, which have separate causes and solutions, together and blames the doctors and suffering patients. Apparantly we’re much easier and defenseless targets compared to the drug dealers and drug abusers that violate the law.
The government and the media are dishonestly conflating prescription OD deaths with illlicit opiate deaths. This needs to stop.
http://www.jpands.org/vol23no1/lilly.pdf
The government and the media are dishonestly conflating prescription OD deaths with illlicit opiate deaths. This needs to stop.
http://www.jpands.org/vol23no1/lilly.pdf
Attachments
Last edited: