- Joined
- Sep 13, 2021
- Messages
- 2,023
- Reaction score
- 2,263
Simul's twitter bio says 'in transit' now. he could be going to cleveland to take Dan's job.

This is literally the reason I never considered Cleveland for school, training, or work.I'd say things are going better for you, both online and IRL
View attachment 348531
View attachment 348530
It would be even worse with no condimentsThis is literally the reason I never considered Cleveland for school, training, or work.
I went to Cleveland once. I haven't returned to Ohio in the 20 subsequent years after that visit.
Well, he CAN care less about accolades. He can care a lot less.
I interviewed at the Cleveland Clinic for residency in the dead of winter after spending all my life in the South. Taking public transportation from the airport to downtown Cleveland felt like taking a train trip through Mordor. Desolation everywhere.This is literally the reason I never considered Cleveland for school, training, or work.
I went to Cleveland once. I haven't returned to Ohio in the 20 subsequent years after that visit.
Having trained in the northeast, I think there’s something to the desolation and academic productivity. Fewer distractions I suppose.I interviewed at the Cleveland Clinic for residency in the dead of winter after spending all my life in the South. Taking public transportation from the airport to downtown Cleveland felt like taking a train trip through Mordor. Desolation everywhere.
Having spent time in nearly every state in the country -Having trained in the northeast, I think there’s something to the desolation and academic productivity. Fewer distractions I suppose.
I took that same train to both CC and Case.I interviewed at the Cleveland Clinic for residency in the dead of winter after spending all my life in the South. Taking public transportation from the airport to downtown Cleveland felt like taking a train trip through Mordor. Desolation everywhere.
I really, really respect you @Mandelin Rain. But, Sriracha for Indian food hurts my heart. Truly.Sriracha for Indian (and some Thai) food. Franks for Buffalo flavored stuff. Cholula for breakfast stuffs. Trader Joe’s Habenero for most anything else.
😉Simul's twitter bio says 'in transit' now. he could be going to cleveland to take Dan's job.
I learned of the delight of Sriracha and Indian food from an Indian doc, who “put that **** on everything”.I really, really respect you @Mandelin Rain. But, Sriracha for Indian food hurts my heart. Truly.
I know there are many Indians here (this is #radonc of course). I can understand some spicy Maggi, aachar (obviously), even chili crisp. But, Sriracha?
I'm not sure how to even proceed.
Ranks even below using usurped taco bell fire sauce in the sauce drawer. Every Indian has oneI really, really respect you @Mandelin Rain. But, Sriracha for Indian food hurts my heart. Truly.
I know there are many Indians here (this is #radonc of course). I can understand some spicy Maggi, aachar (obviously), even chili crisp. But, Sriracha?
I'm not sure how to even proceed.
"Mistake on the lake"This is literally the reason I never considered Cleveland for school, training, or work.
I went to Cleveland once. I haven't returned to Ohio in the 20 subsequent years after that visit.
We have Taco Bell sauce drawer, like Koreans have kimchi fridge (which I have, as well) and Chinese with wok rooms.Ranks even below using usurped taco bell fire sauce in the sauce drawer. Every Indian has one
I would rather go to my local community cancer doctor for a couple of weeks for palliative radiation, than go to MSKCC, get a single fraction treatment, and then get a $45,000 bill for "services not covered" under my PPO.I’m sure the cost of care is less at MSKCC
Anonymously shared with me... Spratt just keeps sounding more and more like a class act9:30
Dan Spratt: "You have to really ask yourself are you doing this because you want to achieve impact in this world? The byproduct of impact, sure, as you've heard, I have papers and grants, I have a good salary, I might have been recognized for things, but those are byproducts and I can care less what my CV looks like. I do it for the impact and these things come with it."
Also Dan Spratt: I've changed multiple national guidelines and work w/ NCI, NRG, CMS, FDA, & pharma, I'm kind of a big deal
Did you guys catch the ketchup reference. Can you trust a man who hates mustard. (8:28)
Anonymously shared with me... Spratt just keeps sounding more and more like a class act
That long?Over/Under on his shelf life? 3 years? 2?
Eat clen, tren hard.if you talk to anyone who overuses T, you will find out that you need to come off the T for a bit. Terrible crash I hear but it is necessary. During this cycle you take anastrozole. Less roid rage, i hear. Some folks may want to take the hand off the T.
Eat clen, tren hard.

Jesus, whos texting at 6 am? These must be people that don't sleep as opposed to people who sleep 8 hrs a night and still get things done bc they don't use condiments and had an elective colostomy.Anonymously shared with me... Spratt just keeps sounding more and more like a class act

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
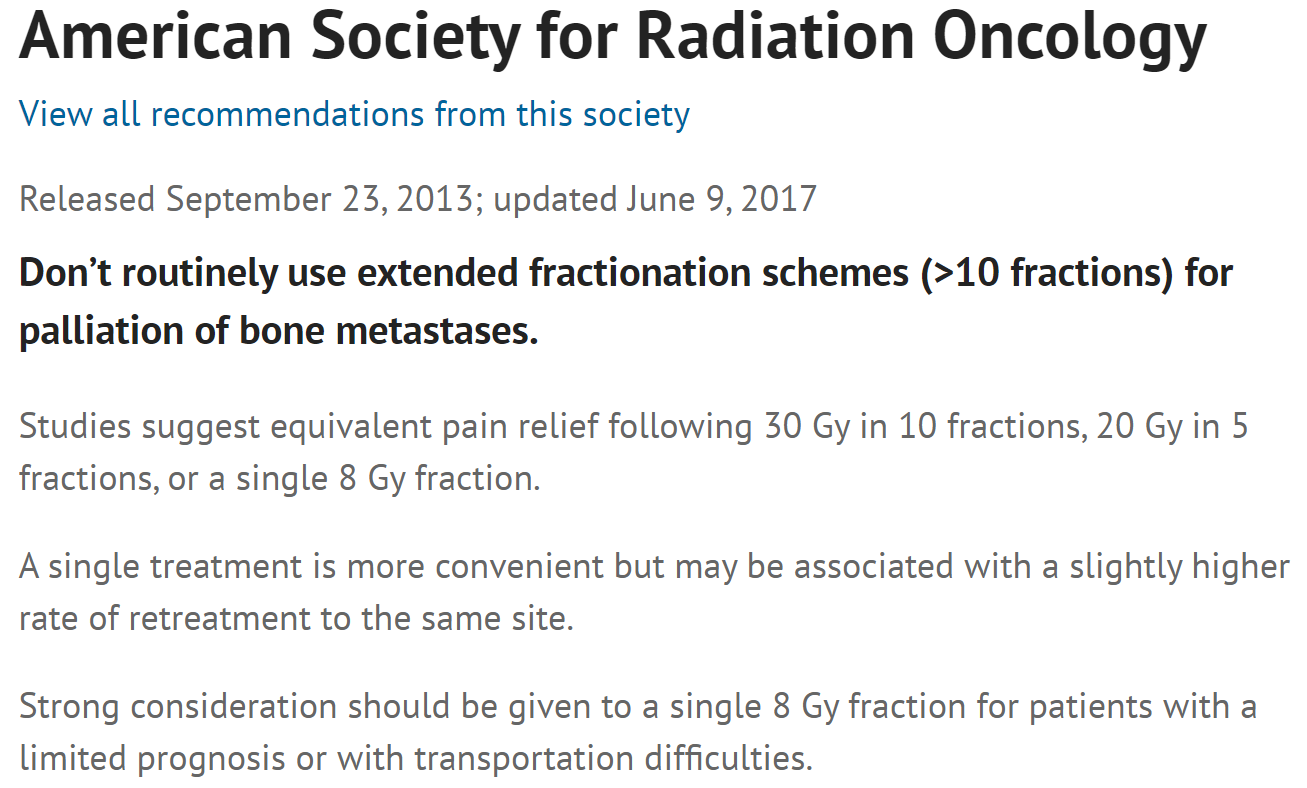
If a RCT is the gold standard, then 30 Gy in 10 fractions is better than 8 Gy x 1 for palliation of bone metastases. Can't have it both ways.
Randomized trial of short- versus long-course radiotherapy for palliation of painful bone metastases - PubMed
Both regimens were equivalent in terms of pain and narcotic relief at 3 months and were well tolerated with few adverse effects. The 8-Gy arm had a higher rate of re-treatment but had less acute toxicity than the 30-Gy arm.
It has same pain control and more acute toxicity - how is it standard ? 😊
Sorry, this is my one hill to die on. The pain control is the same. The re-treatment rate is due to physician’s not believing 8 Gy works AND also less comfort with re-treatment (in the old days) after 30/10 vs after 8/1. Recent meta - analysis showed zero difference in pain scores.
I’m not saying 8/1. Go bigger 10-12 Gy if treating hip or something 3D, 14-16 if treating with conformal or give the Ol’ 24/2 “Canadian bacon” a try !
Canadian bacon... or Canadian bakin' 😉give the Ol’ 24/2 “Canadian bacon” a try !
30/10 vs 12-16 / 1 was done and the single fraction was better …If we want to change the standard of care for bone metastases, then someone should be doing another RCT which helps us clinicians decide which regimen would work best. I'm not saying 30 Gy in 10 fractions is exclusively what I use (it is not), but "RCT is the gold standard" is absolutely a true statement. 30 Gy in 10 fractions vs 12 Gy in 1 fraction vs 24 Gy in 2 fractions: that would be a good RCT.
Remember when we used to do those?
Wasn't SC.24 just published that also showed 24/2 was better for spine mets? Admittedly, it was compared to 20/5 and not 30/1030/10 vs 12-16 / 1 was done and the single fraction was better …
I like to call it "Beggars Can't Be Choosing Wisely."i really think 30/10 is over-utilized, and it is to keep people on beam. I understand this.
I like to call it "Beggars Can't Be Choosing Wisely."
We will never move on.I really think the fx discussion has run its course. The academics have to be right and the pragmatic evil community docs are wrong. Can we all move on now? We don’t need another trial.
This is true.We will never move on.
Dan Spratt will never let his brain and soul admit that single to 5 fraction SBRT palliation at his center can be as expensive as doing 150 standard palliative fractions in 10 patients at an outside community center.
Could you throw the meta-analysis up? Now that I'm out of academia I don't have access to that journal. While this debate was taught to me as not being a debate, I've come to learn that academics have a bent toward proving fewer fractions are better and sometimes create endpoints or inclusion criteria that essentially predetermine the outcome. If 30 in 10 isn't better in certain populations, then I have trouble understanding how SBRT could be better.This is true.
And I’m not an academic zealot. I’m just steadfast on this. I’m not coming from cost point of view. The data shows it is as effective. We have 25 trials showing same pain relief, and recent meta analysis showing same.
But, yes single fraction at Sloan is more $$$ than 10 at free standing. But single fraction at free standing is less than 10 fraction at free standing.
then I have trouble understanding how SBRT could be better.


