- Joined
- May 7, 2014
- Messages
- 1,780
- Reaction score
- 3,833
- Points
- 5,966
- Attending Physician
ABIM salaries are obscene. ABR not as atrocious but check for yourselves.

Sounds familiar with ABR MOC?
ABIM initiated “Choosing Wisely”… much of it centered around cost effectiveness. Ironic!

 www.newsweek.com
www.newsweek.com
Medical Mystery: Making Sense of ABIM's Report
After months of delay, the American Board of Internal Medicine (ABIM) finally filed its latest financial reports with the IRS.
Astro ceo, who have I never hear of earns 650?Medical Mystery: Making Sense of ABIM's Report
After months of delay, the American Board of Internal Medicine (ABIM) finally filed its latest financial reports with the IRS.
An
Astro ceo, who have I never hear of earns 650?
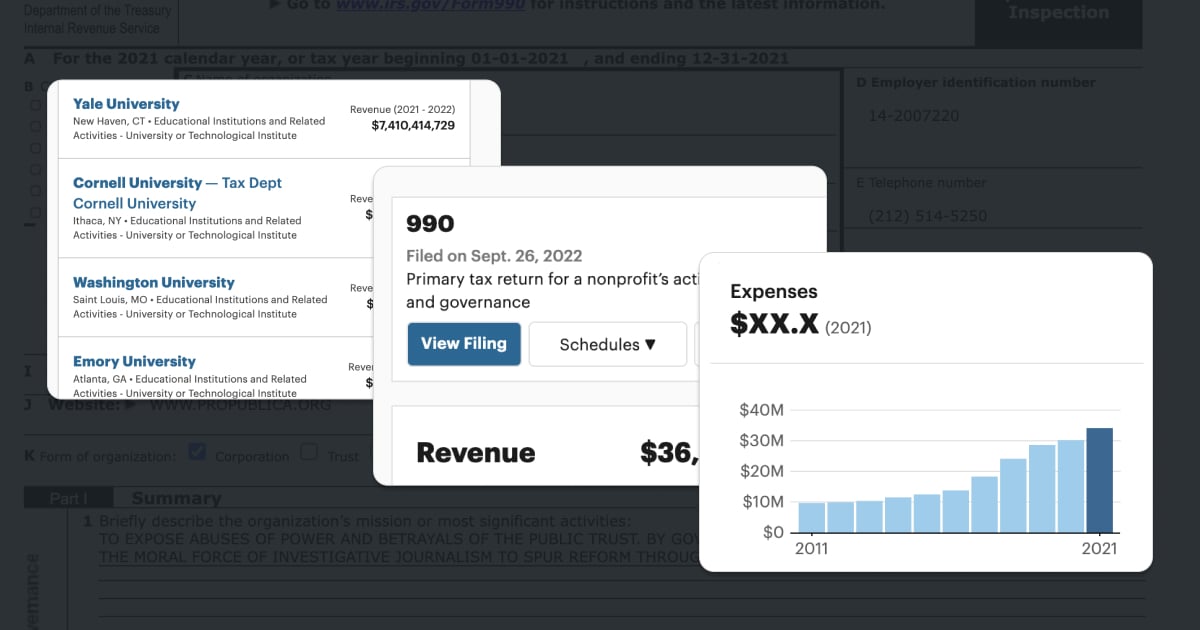
Analagous info for ABR in 2020 attachedAmerican Society For Radiation Oncology, Full Filing - Nonprofit Explorer - ProPublica
Since 2013, the IRS has released data culled from millions of nonprofit tax filings. Use this database to find organizations and see details like their executive compensation, revenue and expenses, as well as download tax filings going back as far as 2001.projects.propublica.org
In 2020 total comp was $750k
American Society For Radiation Oncology, Full Filing - Nonprofit Explorer - ProPublica
Since 2013, the IRS has released data culled from millions of nonprofit tax filings. Use this database to find organizations and see details like their executive compensation, revenue and expenses, as well as download tax filings going back as far as 2001.projects.propublica.org
In 2020 total comp was $750k
Who is this non-md? Has anyone heard of them. Quite a salary to work against our interests.American Society For Radiation Oncology, Full Filing - Nonprofit Explorer - ProPublica
Since 2013, the IRS has released data culled from millions of nonprofit tax filings. Use this database to find organizations and see details like their executive compensation, revenue and expenses, as well as download tax filings going back as far as 2001.projects.propublica.org
In 2020 total comp was $750k


ASTRO might say that is the going rate for a CEO, and they would likely be right. A chair might say 300s starting is “going rate” for a RO, and they might be right! CEO makes over twice as much as many people, but CEOs also didn’t double their numbers. It is simple market economics. Field did it to itself. Just be happy you have A job, “leaders” say.
The ABIM is just greedy, they aren’t actively working to harm the salaries and employment prospects of their members. This is where Astro really distinguishes itself.We all bitch about it but we're better off than what is happening the ABIM. The ABR knows not to push any further.
I'm quite sure the ABR could be easily staffed by willing volunteers only with expenses covered and one plush trip as a reward per year. After all, all the actual WORK that goes into r3tarded things like OLA is done by.. people who like to work for free.
the board is certainly getting their moneys worth and more. Residency expansion/cheap labors and protons are the priorities?It does seem to be the going rate. Sometimes the CEO is an MD though.
And one can always ask, am I getting what I am paying for?
As a member, the answer was no for me, so I dropped my membership.
I wonder if the board thinks they are getting their money’s worth with their CEO?
the board is certainly getting their moneys worth and more. Residency expansion/cheap labors and protons are the priorities?
 www.astro.org
www.astro.org
"You miss 100% of the shots you don't take." - ASTROJust personal opinion, but the board and other prominent non-board members are a lot less cohesive than people might think.
Anyway, anyone can look at their published strategic plan to objectively judge the success of executives and the board. While it is not any one board members fault, I think they collectively do a very bad job on more than half of their stated goals.
Strategic Plan - American Society for Radiation Oncology (ASTRO) - American Society for Radiation Oncology (ASTRO)
ASTRO's strategic plan as outlined on this page, guide the organizations response to the most pressing issues facing the field of radiation oncology.
LOL almost true; they never worked for a university, the lawsuit(s) did not make it to trial, laser center did not get up and running. But I am not arguing with your impressionI quit ASTRO. I encourage everyone to quit ASTRO. As in 100.0% of pp radoncs should stop supporting ASTRO until they stop destroying our field.
ACRO - meh, I don't care for some of the personalities, but at least they pay homage to pp. The fearless leader got a (successful) lawsuit against him for discrimination (university paid) and started a company treating people with "red light" therapy for a bunch of different health issues.. but hey, its all good.
Lots of folks are no longer members, myself included. I tell everyone who asks about it why I'm not an ASTRO member.Mass exodus from Astro would help
But it won’t happen.
the lawsuit(s) did not make it to trial,

Precisely. ITV also an issue.I'm still not sure what that screenshot is pointing out. Bad plan? If he's suggesting the volumes are to big, he should at least give us a pic on lung window.
If we're getting that technical, there was also an old paper, surgical no less, informing ctv decisions by evaluating distance microscopic disease can exist from the primary. I think something like 95% of it in adenos is within 8mm of the primary and within 6 mm in squames (which is not to say I got this big). In any case I do use a ctv, but never do whole lobe rt...Precisely. ITV also an issue.
I’m not sure either. Is that his example of a good plan or a bad plan? Doesn’t seem like enough detail to know. The margins don’t look that big if you figure in windowing and 4DI'm still not sure what that screenshot is pointing out. Bad plan? If he's suggesting the volumes are to big, he should at least give us a pic on lung window.
It's absurd to think it's bad In my estimation. It's not like we get creative. We contour gross disease, account for respiratory motion, make standard expansions and go from there. No offense to Dr stiles, but la-nsclc is one of the more straightforward things we do. Perhaps I should post a pic of a whole right upper lobe sitting on a specimen table and explaining what a travesty it is that theres only a 1 cm adeno in there somewhere.I’m not sure either. Is that his example of a good plan or a bad plan? Doesn’t seem like enough detail to know. The margins don’t look that big if you figure in windowing and 4D
It’s what we do as rad oncs. We btch and complain, fraction/volume/modality shame and wonder why we are at the bottom. All we do is compete with each other to distinguish ourselves to either feed our low levels of self-esteem or to somehow gain an edge against another rad onc to survive.


 www.physiciansweekly.com
www.physiciansweekly.com
At some level/point, i let them go elsewhere if they want to practice medicine/dictate their care (perfect local NCI-designated pps exempt center referral honestly)Perfect example of community practice/"inferior outcomes"/how to think outside the box that they don't teach you in residency is happening today in my world....
I have a p16+ but heavy smoker head/neck guy that doesn't want standard of care treatment. He doesn't want his teeth messed with (refuses pre treatment dental eval) . He's willing to sacrifice efficacy for a chance at better quality of life. He absolutely refuses 70 Gy with weekly Cis. He probably needs a tube but he's refusing it.
I never ran into this at the academic center (partially bcause some of the attendings, not all but some, would just refuse to treat him).
So now do I try to bargain and cut him back to 60 Gy total dose? Consider some neoadj chemo treatment to see if he has a great response then cut dose back (a la the ECOG trial)? Eliminate any elective nodal treatment? Just offer palliative radiation alone to kick the can down the road?
Out in community practice, especially in my area, I swear there is a lot of bargaining patients do. Never saw this in residency.
I have seen cures with treatments that would fail me on boards. But I try to meet people in the middle and some treatment is often better than none. It's a fine line in letting a patient dictate their care to you and trying to get some treatment in to help them and potentially cure them.
At some level/point, i let them go elsewhere if they want to practice medicine/dictate their care (perfect local NCI-designated pps exempt center referral honestly)
Perfect example of community practice/"inferior outcomes"/how to think outside the box that they don't teach you in residency is happening today in my world....
I have a p16+ but heavy smoker head/neck guy that doesn't want standard of care treatment. He doesn't want his teeth messed with (refuses pre treatment dental eval) . He's willing to sacrifice efficacy for a chance at better quality of life. He absolutely refuses 70 Gy with weekly Cis. He probably needs a tube but he's refusing it.
I never ran into this at the academic center (partially bcause some of the attendings, not all but some, would just refuse to treat him).
So now do I try to bargain and cut him back to 60 Gy total dose? Consider some neoadj chemo treatment to see if he has a great response then cut dose back (a la the ECOG trial)? Eliminate any elective nodal treatment? Just offer palliative radiation alone to kick the can down the road?
Out in community practice, especially in my area, I swear there is a lot of bargaining patients do. Never saw this in residency.
I have seen cures with treatments that would fail me on boards. But I try to meet people in the middle and some treatment is often better than none. It's a fine line in letting a patient dictate their care to you and trying to get some treatment in to help them and potentially cure them.
A few folks I know with do multiple courses of quad shot q2 weeksOften enough patients want to ignore my advice. Well ok let's think outside of the box. View it as a natural experiment. Sometimes (more often that I would have thought) works out for them.
For your HN guy might think about 54 in 18. If he refuses even that, SBRT, 44-50 in 5. Every other day or twice a week.
Just had an 80 year old lady that I only treated gross disease.Perfect example of community practice/"inferior outcomes"/how to think outside the box that they don't teach you in residency is happening today in my world....
I have a p16+ but heavy smoker head/neck guy that doesn't want standard of care treatment. He doesn't want his teeth messed with (refuses pre treatment dental eval) . He's willing to sacrifice efficacy for a chance at better quality of life. He absolutely refuses 70 Gy with weekly Cis. He probably needs a tube but he's refusing it.
I never ran into this at the academic center (partially bcause some of the attendings, not all but some, would just refuse to treat him).
So now do I try to bargain and cut him back to 60 Gy total dose? Consider some neoadj chemo treatment to see if he has a great response then cut dose back (a la the ECOG trial)? Eliminate any elective nodal treatment? Just offer palliative radiation alone to kick the can down the road?
Out in community practice, especially in my area, I swear there is a lot of bargaining patients do. Never saw this in residency.
I have seen cures with treatments that would fail me on boards. But I try to meet people in the middle and some treatment is often better than none. It's a fine line in letting a patient dictate their care to you and trying to get some treatment in to help them and potentially cure them.
This is my favorite part of what I like to call...Redneck RadOnc.Out in community practice, especially in my area, I swear there is a lot of bargaining patients do. Never saw this in residency.
I have seen cures with treatments that would fail me on boards. But I try to meet people in the middle and some treatment is often better than none. It's a fine line in letting a patient dictate their care to you and trying to get some treatment in to help them and potentially cure them.
Ok how this? Icu pt on vent. Imported the diagnostic scan into eclipse and drew the field and then brought pt down and used a cone beam/kv to center on carina and give 8 gy off cord without a sim in under 2 hrs totalThis is my favorite part of what I like to call...Redneck RadOnc.
There's what we're taught in the hivemind of the crucible. But the <100 institutions where we all start our training, and the "ASTRO Zeitgeist" in the Red Journal...that's not what's really happening for most of us.
However, it goes in both directions, "good" and "bad" (though I don't believe what we do can be easily labeled in those terms).
At least once a year, and it just happened again this last week, someone will Tweet about doing a "same-day CTSIM with accelerated planning and treatment delivery" like it's a miracle. There are several publications regaling us with tales of such feats.
Except...I've done that many times. The first time, the staff at my small clinic were confused why I was under the impression it wasn't possible. They had no idea that it wasn't routine elsewhere. No one thought it was worth talking about.
Now, the time I did same-day hand calcs for electrons...nah. Never again. Once. One time.
Redneck RadOnc. Sometimes you teach an old man about why you should use soap, sometimes you turn a stellar VMAT plan around in a day. Who knows.
Ok how this? Icu pt on vent. Imported the diagnostic scan into eclipse and drew the field and then brought pt down and used a cone beam/kv to center on carina and give 8 gy off cord without a sim in under 2 hrs total
Does it matter…did emergent RT help? Fortunately, I’m 100% outpatient based so I don’t have to make these decisions.Ok how this? Icu pt on vent. Imported the diagnostic scan into eclipse and drew the field and then brought pt down and used a cone beam/kv to center on carina and give 8 gy off cord without a sim in under 2 hrs total
Does it matter…did emergent RT help?

Used to feel great, doing commando heroic inpt RT on ICU patients, now freestanding, can't treat more than someone with a nasal cannula and honestly i think that's probably for the better based on what I've seen with those really sick pts getting RT, end of life
If anything, I can see the inpatient team blaming radiation for “rapid decompensation following radiation”- radiation pneumonitis is a popular phrase inappropriately used a lot.Treated too many inpatients that died within days to weeks of RT that were so called “emergencies”. Failure to consult the correct specialists
If anything, I can see the inpatient team blaming radiation for “rapid decompensation following radiation”- radiation pneumonitis is a popular phrase inappropriately used a lot.
We have a contract to treat with local hospital. Can't remember the last time we had to use it.Redneck RadOnc uses same-day "sim-plan-treat" because the farmers live an hour away and I'm still the closest linac.
Redneck RadOnc DOES NOT believe in the concept of "emergency radiation".
In fact...Redneck RadOnc might have just responded to an email from MedOnc expressing a similar sentiment, before authoring this post...
Didn’t help, but shouldn’t be in the hospital if he was not getting xrt.Does it matter…did emergent RT help? Fortunately, I’m 100% outpatient based so I don’t have to make these decisions.