- Joined
- Dec 17, 2007
- Messages
- 3,381
- Reaction score
- 4,387
Interesting case today.
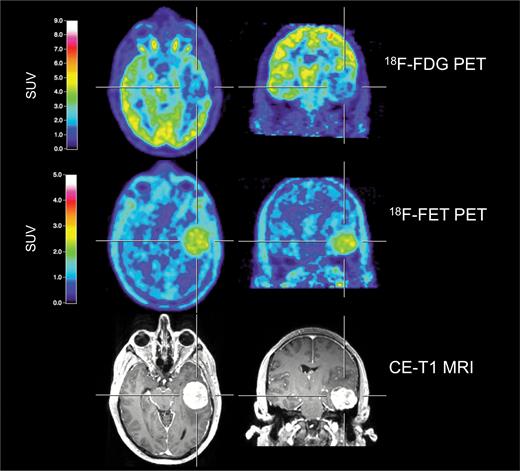
55 year old patient, s/p complete resection of a 4 cm atypical meningeoma 6 years ago (Simpson II).
No adjuvant treatment.
Presents now with a recurrent tumor, about 4mm in size, more or less in the middle of the initial tumor region (apparently some dura was left behind). No symptoms.
Would you treat only the recurrent tumor (SRS/FSRT) or the initial extension?
I would have treated only the recurrent tumor, especially given the long interval since surgery, but it's an atypical one. Thoughts?
55 year old patient, s/p complete resection of a 4 cm atypical meningeoma 6 years ago (Simpson II).
No adjuvant treatment.
Presents now with a recurrent tumor, about 4mm in size, more or less in the middle of the initial tumor region (apparently some dura was left behind). No symptoms.
Would you treat only the recurrent tumor (SRS/FSRT) or the initial extension?
I would have treated only the recurrent tumor, especially given the long interval since surgery, but it's an atypical one. Thoughts?
Last edited:
")