You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.

- Joined
- Mar 22, 2008
- Messages
- 4,130
- Reaction score
- 2,742
- Points
- 6,851
- Location
- Phoenix, Arizona
- Attending Physician
18g cervical and lumbar sometimes 16g lumbar
- Joined
- Apr 10, 2021
- Messages
- 87
- Reaction score
- 85
- Points
- 451
18g lumbar
20g cervical
20g Sidekick genicular
20g cervical
20g Sidekick genicular
- Joined
- May 8, 2004
- Messages
- 4,290
- Reaction score
- 2,016
- Points
- 5,796
- Attending Physician
do you use multiple nimbus needles for lumbar?18 guage for cervical
18 guage nimbus for lumbar
I'm:
20 gauge cervical
18 gauge lumbar
nimbus for SIJ and thoracic
- Joined
- Apr 13, 2016
- Messages
- 3,601
- Reaction score
- 3,748
- Points
- 6,746
- Location
- California
- Attending Physician
18g 10mm curved tip for everything.
- Joined
- Dec 12, 2006
- Messages
- 3,132
- Reaction score
- 3,714
- Points
- 7,451
- Attending Physician
20G 10mm curved for everything
- Joined
- Nov 4, 2004
- Messages
- 1,291
- Reaction score
- 619
- Points
- 6,241
- Attending Physician
16gu for everything not in the neck. 18gu for the neck
- Joined
- May 30, 2005
- Messages
- 23,705
- Reaction score
- 15,310
- Points
- 8,731
- Location
- Canton GA
- Website
- www.stevenlobel.com
- Attending Physician
20g10mm everything except gasserian. 22g5mm
- Joined
- Oct 23, 2005
- Messages
- 8,317
- Reaction score
- 6,059
- Points
- 7,396
- Attending Physician
18G for all facet RFA.
16G for SIJ and peripheral joint RFA
16G for SIJ and peripheral joint RFA
Advertisement - Members don't see this ad
- Joined
- May 30, 2005
- Messages
- 23,705
- Reaction score
- 15,310
- Points
- 8,731
- Location
- Canton GA
- Website
- www.stevenlobel.com
- Attending Physician
Speak softly and carry a big stick.18G for all facet RFA.
16G for SIJ and peripheral joint RFA
- Joined
- Dec 14, 2019
- Messages
- 82
- Reaction score
- 64
- Points
- 411
- Dentist
What technique are you using for SI joint?18G for all facet RFA.
16G for SIJ and peripheral joint RFA
- Joined
- Oct 23, 2005
- Messages
- 8,317
- Reaction score
- 6,059
- Points
- 7,396
- Attending Physician
I should mention that although I used to do a dozen SIJ RFA a year, now I rarely do it except for standard medicare patients because SIJ RFA is covered for them.What technique are you using for SI joint?
Reason is that I see same or superior outcomes doing a combination of IA and periarticular PRP now for the SIJ. It usually lasts for a couple years and usually works better than SIJ RFA. Since both of these SIJ techniques are now cash procedures, patients are much more willing to go for something that heals the issue, instead of just removing the pain temporarily. And it is Actually is much cheaper for patients to do SIJ PRP every couple years instead of SIJ RFA every 8-12 months.
But when I do SIJ RFA, I use a bipolar technique, at each of the three lesion locations at S1, S2, and two S3 locations used for cooled RFA. You can easily look up the cooled RFA technique if you haven't seen it before.
I also use a bipolar technique with 16G needles for all peripheral joint RFA. Works as well as the expensive probes with less cost. It does require an extra cannulae placement and time for genicular RFA (because three nerves), but does work better than standard genicular RFA.
For shoulder and hip RFA, I’m slightly slower but not much, because you’re typically only lesioning two nerves.
Last edited:
- Joined
- Nov 4, 2004
- Messages
- 1,291
- Reaction score
- 619
- Points
- 6,241
- Attending Physician
Any one use that nimbus needle/cannula? Apparently works with all probes. Don’t know the cost, but curious if anyone has insight.
D
deleted875186
Can you elaborate, how do you place the bipolar needles for a genicular ablation?I should mention that although I used to do a dozen SIJ RFA a year, now I rarely do it except for standard medicare patients because SIJ RFA is covered for them.
Reason is that I see same or superior outcomes doing a combination of IA and periarticular PRP now for the SIJ. It usually lasts for a couple years and usually works better than SIJ RFA. Since both of these SIJ techniques are now cash procedures, patients are much more willing to go for something that heals the issue, instead of just removing the pain temporarily. And it is Actually is much cheaper for patients to do SIJ PRP every couple years instead of SIJ RFA every 8-12 months.
But when I do SIJ RFA, I use a bipolar technique, at each of the three lesion locations at S1, S2, and two S3 locations used for cooled RFA. You can easily look up the cooled RFA technique if you haven't seen it before.
I also use a bipolar technique with 16G needles for all peripheral joint RFA. Works as well as the expensive probes with less cost. It does require an extra cannulae placement and time for genicular RFA (because three nerves), but does work better.
- Joined
- Oct 7, 2011
- Messages
- 17,076
- Reaction score
- 7,454
- Points
- 8,401
- Attending Physician
if your SIJ PRP is healing the condition, why do they need repeat injections 2 years out?
i assume you mean the PRP is healing younger patients, not those with chronic SI joint pain and end stage arthritis, because i have not seen any evidence that any injection heals bony arthritis.
i assume you mean the PRP is healing younger patients, not those with chronic SI joint pain and end stage arthritis, because i have not seen any evidence that any injection heals bony arthritis.
- Joined
- Apr 26, 2002
- Messages
- 3,097
- Reaction score
- 1,623
- Points
- 6,611
- Website
- na.com
- Attending Physician
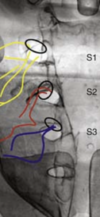
nvrsumr modified approach. I have tried alot of different approaches over last 10+ years. 18g everything: palisade bipolar, add L5 dorsal ramus, multiple needles/burns medial to foramen.
I now place as in attached images and do single lesion for 90s at 90C with 22g.
I am doing more of these than ever with greater success than any of the other options above. Have never done cooled rf though.
I now place as in attached images and do single lesion for 90s at 90C with 22g.
I am doing more of these than ever with greater success than any of the other options above. Have never done cooled rf though.
Attachments


- Joined
- May 8, 2004
- Messages
- 4,290
- Reaction score
- 2,016
- Points
- 5,796
- Attending Physician
Any one use that nimbus needle/cannula? Apparently works with all probes. Don’t know the cost, but curious if anyone has insight.
I use them. I’m told they’re $75 a piece.
I do a bipolar strip lesion for SIJ and use MM’s targets for thoracic RFA with the nimbus needles.
- Joined
- Nov 28, 2011
- Messages
- 2,722
- Reaction score
- 1,749
- Points
- 6,761
- Location
- New Jersey
- Attending Physician
nvrsumr modified approach. I have tried alot of different approaches over last 10+ years. 18g everything: palisade bipolar, add L5 dorsal ramus, multiple needles/burns medial to foramen.
I now place as in attached images and do single lesion for 90s at 90C with 22g.
I am doing more of these than ever with greater success than any of the other options above. Have never done cooled rf though.
I’m intrigued by your reported results. In what view do you place the needles and what are your targets? 22 ga cannula for 90s is not creating a sizable lesion but you are laying the length of the active tip on bone. Either your have successfully precisely located the lateral branches or this hurts so much less than more common techniques that patients are happy.
- Joined
- Apr 26, 2002
- Messages
- 3,097
- Reaction score
- 1,623
- Points
- 6,611
- Website
- na.com
- Attending Physician
Appreciate the interest. Not lightening in a bottle.
Needle insertion caudal to get cannulae tips parallel to os in final placement.
I have a cephalad tilt to the II and oblique as necessary to see S1, S2 and S3 posterior foramina and groove the nerve exits in laterally. From anatomical pictures the branching of the of the nerves is less medially and inferiorly for S1, midline S2 and superior S3. This is where I put the tips of the needles. Snug against OS ventral, tip firmly against superior wall of the groove for S3 and usually S2. S1 I am inferior for placement.
Go to lateral. Often looks a bit different than the fluoro image in previous post. The sacrum is triangle in lateral view and usually S2 and S3 are lower on the slope so your needle appears to be almost in sacral canal. If I see this at SI I am too ventral and not a safe placement. This allows me to place more medial safely in AP for S1 which gets me closer to where it branchs. I believe S1 is largest and provides most innervation to joint so I am particular about placement.
As far as lesion size a 22g lesion is 6x10 versus 7.5x12mm for 18g. When I did bipolar palisade with 18 had terrible patient post procedural discomfort that limited adoption. I get a similar phenomenon to medial branch neuritis infrequently but well tolerated otherwise.
Just my anecdotal experience.
Needle insertion caudal to get cannulae tips parallel to os in final placement.
I have a cephalad tilt to the II and oblique as necessary to see S1, S2 and S3 posterior foramina and groove the nerve exits in laterally. From anatomical pictures the branching of the of the nerves is less medially and inferiorly for S1, midline S2 and superior S3. This is where I put the tips of the needles. Snug against OS ventral, tip firmly against superior wall of the groove for S3 and usually S2. S1 I am inferior for placement.
Go to lateral. Often looks a bit different than the fluoro image in previous post. The sacrum is triangle in lateral view and usually S2 and S3 are lower on the slope so your needle appears to be almost in sacral canal. If I see this at SI I am too ventral and not a safe placement. This allows me to place more medial safely in AP for S1 which gets me closer to where it branchs. I believe S1 is largest and provides most innervation to joint so I am particular about placement.
As far as lesion size a 22g lesion is 6x10 versus 7.5x12mm for 18g. When I did bipolar palisade with 18 had terrible patient post procedural discomfort that limited adoption. I get a similar phenomenon to medial branch neuritis infrequently but well tolerated otherwise.
Just my anecdotal experience.
Attachments
Last edited:
Advertisement - Members don't see this ad
- Joined
- Apr 2, 2010
- Messages
- 475
- Reaction score
- 176
- Points
- 4,991
- Attending Physician
If there is a procedure I hate doing it would be SIJ cRFA. Really tedious. Since there is less tissue overlying the sacrum the cannulas never have proper purchase so they flop around all the time. And, there are so many locations to lesion. Also, I don't always get good results.I should mention that although I used to do a dozen SIJ RFA a year, now I rarely do it except for standard medicare patients because SIJ RFA is covered for them.
Reason is that I see same or superior outcomes doing a combination of IA and periarticular PRP now for the SIJ. It usually lasts for a couple years and usually works better than SIJ RFA. Since both of these SIJ techniques are now cash procedures, patients are much more willing to go for something that heals the issue, instead of just removing the pain temporarily. And it is Actually is much cheaper for patients to do SIJ PRP every couple years instead of SIJ RFA every 8-12 months.
But when I do SIJ RFA, I use a bipolar technique, at each of the three lesion locations at S1, S2, and two S3 locations used for cooled RFA. You can easily look up the cooled RFA technique if you haven't seen it before.
I also use a bipolar technique with 16G needles for all peripheral joint RFA. Works as well as the expensive probes with less cost. It does require an extra cannulae placement and time for genicular RFA (because three nerves), but does work better than standard genicular RFA.
For shoulder and hip RFA, I’m slightly slower but not much, because you’re typically only lesioning two nerves.
But I do want to get my patient pain relief when SIJ injections don't last. Which leads me to...there is a bipolar version of the cRFA technique? I think strip lesions are the way to go with SIJ RFAs so I would be interested in learning more. Have never tried bipolar in general. I have two RF generators at my hospital. One is a Kimberly Clark which is compatible with my cRFA kits. The other is a Medtronic Accurian which is not. Would these work?
- Joined
- Feb 13, 2016
- Messages
- 93
- Reaction score
- 62
- Points
- 4,931
- Location
- Minneapolis, MN
- Attending Physician
Anyone doing thermal hip? I would appreciate any advice/images.
- Joined
- Jul 27, 2009
- Messages
- 1,813
- Reaction score
- 1,129
- Points
- 5,621
If there is a procedure I hate doing it would be SIJ cRFA. Really tedious. Since there is less tissue overlying the sacrum the cannulas never have proper purchase so they flop around all the time. And, there are so many locations to lesion. Also, I don't always get good results.
But I do want to get my patient pain relief when SIJ injections don't last. Which leads me to...there is a bipolar version of the cRFA technique? I think strip lesions are the way to go with SIJ RFAs so I would be interested in learning more. Have never tried bipolar in general. I have two RF generators at my hospital. One is a Kimberly Clark which is compatible with my cRFA kits. The other is a Medtronic Accurian which is not. Would these work?
The only bipolar cooled RF systems I've heard of are the Medtronic Osteocool for Bone ablation which is a bipolar lesion on a single electrode and the Avanos/Coolief Biaculoplasty kit. I don't think the Avanos one is a true bipolar/cross talk though, as I think it's a really just two monopolar lesions that interact.
The monopolar dual electrode kit for Avanos does make the case go faster, but I hate the SIJ RFA.
I may try the approach above from nvrsumr as that looks like a poor man's SI-Simplicity and maybe add in a second path a touch more lateral to create a wider lesion.
- Joined
- Apr 13, 2016
- Messages
- 3,601
- Reaction score
- 3,748
- Points
- 6,746
- Location
- California
- Attending Physician
Palisade technique.If there is a procedure I hate doing it would be SIJ cRFA. Really tedious. Since there is less tissue overlying the sacrum the cannulas never have proper purchase so they flop around all the time. And, there are so many locations to lesion. Also, I don't always get good results.
But I do want to get my patient pain relief when SIJ injections don't last. Which leads me to...there is a bipolar version of the cRFA technique? I think strip lesions are the way to go with SIJ RFAs so I would be interested in learning more. Have never tried bipolar in general. I have two RF generators at my hospital. One is a Kimberly Clark which is compatible with my cRFA kits. The other is a Medtronic Accurian which is not. Would these work?