- Joined
- Apr 13, 2012
- Messages
- 908
- Reaction score
- 246
- Points
- 5,291
- Attending Physician

Super true especially the first part. Icu course is so long any psychological trauma of a light intubation will be overwritten by the horrors of being critically I’ll, proned, rectal tube etc etc. I always shoot lighter that the crazy doses I read about (eg 0.3 mg/kg etomidate, 2 mg/kg protocol etc). I do switch up my amnestic agent to try to stay versatile with dousing but I usually use roc to help with lines and initial vent management.Coming from anesthesia/cc background. These patients are generally not going to remember anything significant given their shock state, hypoxia, acidosis, brain trauma, or whatever bad reason they need a crashing intubation. So hypnotic choice isn’t so important in my opinion. Give less, you could always give more. They’d rather be alive than dead.
Versed 2-4 mg followed by roc is my general go to. Propofol if I have it 30mg with NE bolus. Etomidate about 6-10mg, maybe my least favorite but it’s readily available since it’s not narcotic. Ketamine for asthma/copd is nice. Rocuronium is my go to paralytic, gives about an hour of paralysis to get lines in easy, check vent pressures, etc. I’d consider sux for super obese pts where dosing is more reliable based on body weight but I’m sure pounding 200mg roc would put anyone down too. In any case, I always try to have some upper push dose sticks (NE, epi, phenyl, etc) and some downer (esmolol) with me along with the RSI meds.
Sometimes i’ll push versed/fentanyl and peak at the cords, if its open I place the tube. Am I too barbaric for this? A propfol gtt will be hanging immediately ready to go, as well as levophed gtt.
If not sedated enough, add some propofol +/- roc. If hypotensive, etomidate + roc.
Not much experience with ketamine for intubating, I’m assuming folks will push some versed followed by ketamine ? Please do share.
I don’t believe that etomidate “doesn’t effect BP” which doesn’t mean it’s a bad or wrong drug to use. Ketamine seems to effect BP less as long as it’s not slammed in. If it’s not slammed in patients will also continue to spontaneously breath nicely and you can usually keep on any PAP until your paralytic kicks in.
I don’t know that you are barbaric. I think there are many ways to skin this cat. And we all have to do what seems the most reasonable and we are comfortable with based on experience. I personally don’t like “peeky peeks” personally seen too much gagging and gastric contents into the airway than I ever want to again. I a big believer that while paralytics do take you into “no man’s land” they drastically improve first pass success and I don’t look until I’m ready to place a tube these days with a paralytic active. I have partners that (almost) never paralyze. You can find strong opinions either way.
I like a bit of versed often before to calm any anxiety and stop the memory formations.
True.
Do you use roc or sux ?
Usually sux as long as that choice wouldn’t be great.
What do you mean wouldn’t be great?
Myasthenia is not a contraindication to sux, you just need a good dose to be effectiveA patient with high K or myasthenia for instance.
Myasthenia is not a contraindication to sux, you just need a good dose to be effective
Rhabdo or seizures would prob be a contraindicationMyasthenia is not a contraindication to sux, you just need a good dose to be effective
I wouldn’t call seizures a contraindication, in fact prefer it because I want to see if they’re still seizing or not after they’ve been intubated (minimal access to continuous eeg)Rhabdo or seizures would prob be a contraindication
Which are these studies that show sux superiority?Multiple studies have consistently shown succinylcholine to be superior to rocuronium. I don’t understand why some pulm/cc physicians are so afraid of sux and even paralytics in general.

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
 jamanetwork.com
jamanetwork.com
I’m just use to using roc from my training. I want to be more comfortable using sux thoughMultiple studies have consistently shown succinylcholine to be superior to rocuronium. I don’t understand why some pulm/cc physicians are so afraid of sux and even paralytics in general.
The first study shows no difference when you take high dose roc into account.Rocuronium versus succinylcholine for rapid sequence induction intubation - PubMed
Succinylcholine created superior intubation conditions to rocuronium when comparing excellent intubation conditions. Using the less stringent outcome, clinically acceptable intubation conditions, the two agents were not statistically different. Intubation conditions were not statistically...
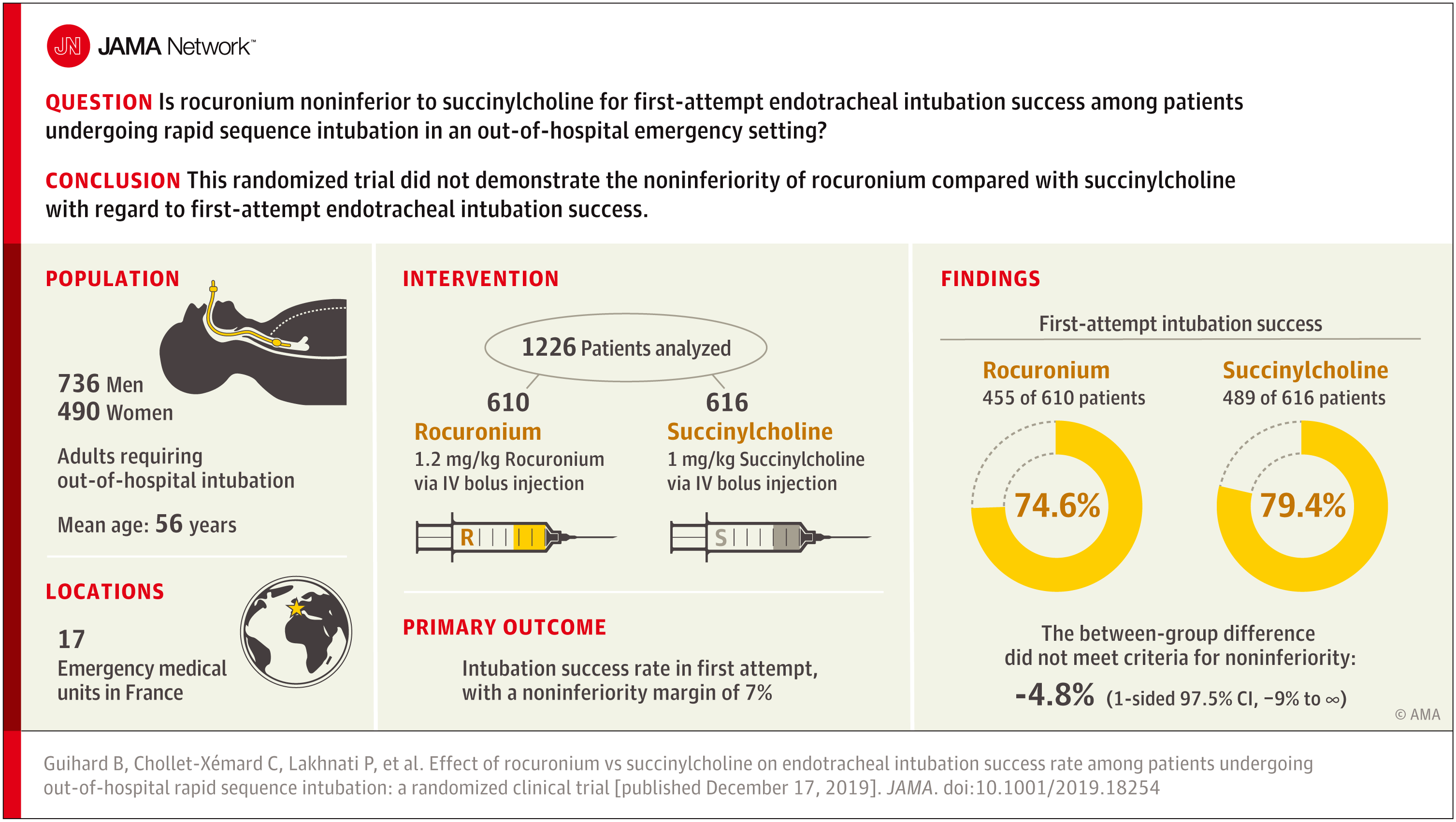
Effect of Rocuronium vs Succinylcholine on Successful Out-of-Hospital Rapid Sequence Intubation
This noninferiority trial compares the effect of rocuronium vs succinylcholine on first-attempt tracheal intubation success rate in out-of-hospital emergency situations among patients undergoing rapid sequence intubation.
Multiple studies have consistently shown succinylcholine to be superior to rocuronium. I don’t understand why some pulm/cc physicians are so afraid of sux and even paralytics in general.
It seems to me that I get a better view of cords with succinycholine.
Rocuronium versus succinylcholine for rapid sequence induction intubation - PubMed
Succinylcholine created superior intubation conditions to rocuronium when comparing excellent intubation conditions. Using the less stringent outcome, clinically acceptable intubation conditions, the two agents were not statistically different. Intubation conditions were not statistically...
Effect of Rocuronium vs Succinylcholine on Successful Out-of-Hospital Rapid Sequence Intubation
This noninferiority trial compares the effect of rocuronium vs succinylcholine on first-attempt tracheal intubation success rate in out-of-hospital emergency situations among patients undergoing rapid sequence intubation.
ExactlyYou get the same intubation conditions (aka degree of muscle relaxation) by waiting a few more seconds after giving high dose roc. It also gives you more prolonged apnea time before desaturation. And you don't have to worry about thr nasty side effects and contraindications that exist with suxx. I almost exclusively use high dose roc for RSI
I use them both. But I don’t always paralyze, about 80% of the time. I get a lot of hypercapnics, and Neuro pats that don’t need much.Multiple studies have consistently shown succinylcholine to be superior to rocuronium. I don’t understand why some pulm/cc physicians are so afraid of sux and even paralytics in general.
This is generally my practice as wellI don't think there's any significant difference between the drug choices, when used properly.
I generally use midazolam 2-4mg for amnesia, plus/minus propofol for hypnotic, then rocuronium 1.2mg/kg.
I always paralize unless there it is an obvious difficult intubation and likely difficult ventilation. Even then, the improved view etc might still nudge me to sux or roc-sugammadex. RE. roc vs sux - they both work the same, sux is dirtier, roc is longer acting, slower onset. When people say sux works better, they are basically saying they lack patience and cant wait a minute for the drug to work.
I also always have a bag of LR and norepi either primed & ready, or actively being mixed in the background.
NoLet's make this interesting.
Except for the novices and those who are uncomfortable with recovery requiring LMA or a cric, is there any reason to not use 2 per kg roc over any dose of sucks?
HH
--If there's a bad outcome, they'll come for you at peer review /s.Let's make this interesting.
Except for the novices and those who are uncomfortable with recovery requiring LMA or a cric, is there any reason to not use 2 per kg roc over any dose of sucks?
HH
Not readily available, no. I'd need to call anesthesia on call to bring it to bedside. In my practice, I would need to diagnose the patient as high risk cannot intubate/cannot ventilate, and has contraindication for sux.Do you guys have sugammadex readily available in the unit? It has definitely changed the roc/sux discussion in anesthesia, if you DO get into trouble after paralysis.
Though when you intubate someone, it’s not like returning to spontaneous ventilation is a great choice. There’s a reason you were tubing them in the first place.
Histamine release is only associated with the benzylisoquinolinium NMDBs, more specifically atracurium & mivacurium. It's a chemical structure thing. Sux, cisatracurium and the aminosteroids may cause more typical allergic reaction; sux > benzylisos > aminosteroids.--If there's a bad outcome, they'll come for you at peer review /s.
I literally can't think of any. Is there any literature on histamine release w/ high dose roc (more of a concern with aminosteroids)? I tried to search a little but I'm not seeing any reports of it. Logistically, it might cause a delay when the nurse has to go back to the pyxis for a third, then fourth, vial.
The suga is only tested/dosed for rescue of 1.2mg/kg……😉Let's make this interesting.
Except for the novices and those who are uncomfortable with recovery requiring LMA or a cric, is there any reason to not use 2 per kg roc over any dose of sucks?
HH
septic shock with BPs in the 60s etc
Bad combo.Propofol
I mentioned that I do most of my tubes with just etomidate in a different thread and people were outright horrified at my malpractice of not paralyzing.Anesthesia Critical Care here... underappreciated is the role of the un-induced intubation. Why is an RSI being chosen?
Severe hypoxemia? Why not maintain spontaneous ventilation on HFNC while you intubate?
Full stomach or propensity to aspirate? Why not maintain consciousness and airway reflexes while intubating?
Perceived difficult mask ventilation? Why mask at all if the patient continues ventilating during intubation?
Because most people that sick have crappy spont efforts after just the induction agent that are more of a hindrance than a helpAnesthesia Critical Care here... underappreciated is the role of the un-induced intubation. Why is an RSI being chosen?
Severe hypoxemia? Why not maintain spontaneous ventilation on HFNC while you intubate?
Full stomach or propensity to aspirate? Why not maintain consciousness and airway reflexes while intubating?
Perceived difficult mask ventilation? Why mask at all if the patient continues ventilating during intubation?
Right, but I'm not talking about inducing without paralysis; I'm talking about not inducing at all. HFNC or bipap, topical, glide.Because most people that sick have crappy spont efforts after just the induction agent that are more of a hindrance than a help
Because aspiration is less likely when the pt is paralysed
Because mask ventilation is easiest with the pt paralysed and true difficult mask ventilation with two hands and an OPA is exceedingly rare
If the pt is so obtunded, encephalopathic, or they have 1/2 MAC of CO2 I think that’s completely reasonable. Why burn a bridge you don’t have to. In these scenarios their medical/metabolic condition is the anesthetic.Right, but I'm not talking about inducing without paralysis; I'm talking about not inducing at all. HFNC or bipap, topical, glide.