- Joined
- Jan 31, 2010
- Messages
- 805
- Reaction score
- 1,081

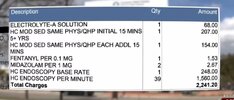
SA man says hospital forgot to sedate him during procedure, and he has a drug screening to prove it
A San Antonio man who said a hospital failed to sedate him during an outpatient procedure last fall went as far as to get an independent drug screening to prove the powerful drugs were not in his system.
I am leaning toward him not having received the medication if he had gone to an independent facility and tested negative for both opioids and benzos with a 6 hour window. 2 false negatives in a sample is rare.
Other potential possibility is he is running a scam with adulterated urine sample or non-own sample in order to setup for a lawsuit....but that's pretty out there and assuming some level of understanding of usual drugs used in Mac anesthesia settings, detection windows etc.
 . For a large man like this patient I don't have a hard time believing that he indeed was pretty much fully awake for the colonoscopy, even if those those wimpy doses were in fact given... especially if perhaps he has a bit of a "healthy metabolism" (MJ or EtOH use).
. For a large man like this patient I don't have a hard time believing that he indeed was pretty much fully awake for the colonoscopy, even if those those wimpy doses were in fact given... especially if perhaps he has a bit of a "healthy metabolism" (MJ or EtOH use).