- Joined
- Jan 2, 2009
- Messages
- 1,435
- Reaction score
- 346

It’s interesting to see the push for more mid level care providers portrayed in a negative light by the media for once. It seems like usually the spin is that mid levels need to be freed from the tyranny of the greedy physicians.
I guess the PE bankers are among the few professions the media despises more than physicians.
The public is dumb but if there’s one thing they hate it’s Wall Street. If it’s being done by PE, then It must be bad regardless. So for once this works to our advantage.
Same can be true of anesthesia. With glidescopes and ultrasound. You can teach any ******* basics of procedure skills in anesthesia in 6 months to be honest. I’m not kidding. I felt comfortable with omfs residents after they had 4 months under their belt to be in room alone for most of the cases.We aren’t next. EM residency is 3 years and the majority of what they do is simple complaints, managing social issues, and non procedural. Algorithms all very commonly used in EDs.
Most of us have done 5+ years of training and most crnas want nothing to do with indepedent practice.
EM is imminently replaceable because of the nature of their work. Fully 3/4 of a normal ED is drunks sleeping off a bender, sniffles or coughs, acute abdominal pain, or simple lacs.
You’re obviously gonna need doctors to stabilize traumas and severe sepsis, but that other stuff can and should be farmed out if you ask me.
You felt comfortable because you know how to bail them out of trouble and OMFS residents will actually call you before **** gets bad.Same can be true of anesthesia. With glidescopes and ultrasound. You can teach any ******* basics of procedure skills in anesthesia in 6 months to be honest. I’m not kidding. I felt comfortable with omfs residents after they had 4 months under their belt to be in room alone for most of the cases.
It’s a different world we live in these days. With fake online nursing degrees getting into the real world working as well.
Not if it’s me under the knife.Same can be true of anesthesia. With glidescopes and ultrasound. You can teach any ******* basics of procedure skills in anesthesia in 6 months to be honest. I’m not kidding. I felt comfortable with omfs residents after they had 4 months under their belt to be in room alone for most of the cases.
It’s a different world we live in these days. With fake online nursing degrees getting into the real world working as well.
On the IQ and got-their-****-together bell curves, OMFS residents are faaaaaar to the right of the NP-wannabes. Yeah, you can make a good CA1 out of an OMFS resident (for appropriately selected cases) but I don't get where you think that level of trainability translates to the pool of nurses who want to be NPs.I felt comfortable with omfs residents after they had 4 months under their belt to be in room alone for most of the cases.
“Once he had placed 10 tubes under a doctor's supervision, he would be allowed to do it on his own”
Yeah, we’re part of the problem. Have some shame and dignity and don’t train your replacement.
Yeah, I heard that if a dental class has 150-200 students, 2-3 might get OMFS, 2 might get orthodontics, and 2 might get endodontics. Then the rest are generalists. I may not have all of the specialties and numbers exactly correct, but the numbers are in the 1-3 range for all subs. So, OMFS are the cream of the crop.On the IQ and got-their-****-together bell curves, OMFS residents are faaaaaar to the right of the NP-wannabes. Yeah, you can make a good CA1 out of an OMFS resident (for appropriately selected cases) but I don't get where you think that level of trainability translates to the pool of nurses who want to be NPs.
OMFS is populated by one of the most talented and driven cohorts of people in healthcare. Yeah. They do great. Of course they do. So what?
I hope you are wrong.Same can be true of anesthesia. With glidescopes and ultrasound. You can teach any ******* basics of procedure skills in anesthesia in 6 months to be honest. I’m not kidding. I felt comfortable with omfs residents after they had 4 months under their belt to be in room alone for most of the cases.
It’s a different world we live in these days. With fake online nursing degrees getting into the real world working as well.
“Once he had placed 10 tubes under a doctor's supervision, he would be allowed to do it on his own”
Yeah, we’re part of the problem. Have some shame and dignity and don’t train your replacement.
10 chest tubes is honestly a lot more than i expected ...
This chart below is what came up when i googled procedural requirements for EM residents. it also says 10 chest tubes minimum. (im surprised they are required to do 3 crics... thats a lot of crics if each resident needs 3 minimum!)
View attachment 366188
Same can be true of anesthesia. With glidescopes and ultrasound. You can teach any ******* basics of procedure skills in anesthesia in 6 months to be honest. I’m not kidding. I felt comfortable with omfs residents after they had 4 months under their belt to be in room alone for most of the cases.
It’s a different world we live in these days. With fake online nursing degrees getting into the real world working as well.
You know who likely has more money and lobbying power? Insurance companies and large hospital systems. The recent studies showing NPs costing hospitals and insurance companies more for the same level of care is a huge red flag and this evidence should be put to good use. My hope is that insurers and hospitals wake up and realize they are shooting themselves in the foot by hiring mid levels who follow inefficient algorithms rather than use their brain.PEs are rich. they lobby their way out of almost anything.
also they dont care about the patients that get injured. they tend to be the poor. the rich patients will obviously get the doctor to care for them. its unfortunate.
That rationalization has never worked for them. We see this every day at the patient level when drugs with enormous benefit (wegovy, entresto) are denied due to that expense even though keeping the patient out of the hospital even a single time would be worth decades of prescription costs. Or when someone on crappy insurance can't get discharged and the hospital refuses to eat the cost as a charity case and their acute care bed sits there unusable for months.You know who likely has more money and lobbying power? Insurance companies and large hospital systems. The recent studies showing NPs costing hospitals and insurance companies more for the same level of care is a huge red flag and this evidence should be put to good use. My hope is that insurers and hospitals wake up and realize they are shooting themselves in the foot by hiring mid levels who follow inefficient algorithms rather than use their brain.
Yeah, I heard that if a dental class has 150-200 students, 2-3 might get OMFS, 2 might get orthodontics, and 2 might get endodontics. Then the rest are generalists. I may not have all of the specialties and numbers exactly correct, but the numbers are in the 1-3 range for all subs. So, OMFS are the cream of the crop.
Perhaps. But I assume they study a very different curriculum than a med student, so, as you said, they are very different. I think it would be unfair to compare them to Fam Medicine resident USMLE scores if they did not receive the full curriculum needed to prepare for the USMLE. It seems like it would be like me taking a biology course but taking the test for a biochem course. They are kind of related but definitely not the same. All that being said, I don't know much about what they study. My only point was that, to get into one of those subs, they had to be in the top 2-3% of a fairly competitive bunch of students. Just getting into dental school is competitive and then you skim the top couple percent off of that group and you likely are dealing with some pretty bright, motivated, and competitive candidates.Probably, but I was told they take a slightly less difficult USMLE step 1 version to get into OMFS (MD program) and the average score of the ones who got in is lower than FM residents step1 score. You are comparing different cohort of students.
Probably, but I was told they take a slightly less difficult USMLE step1 version (CBSE) to get into OMFS (MD program) and the average score of the ones who got in is lower than FM residents step1 score. You are comparing different cohort of students.
Based on the dental forum, a 75 (or 223) is a GREAT score. 70 (or 213) is a competitive score.
My point was that it is tricky to compare these 2 different cohort of students.Perhaps. But I assume they study a very different curriculum than a med student, so, as you said, they are very different. I think it would be unfair to compare them to Fam Medicine resident USMLE scores if they did not receive the full curriculum needed to prepare for the USMLE. It seems like it would be like me taking a biology course but taking the test for a biochem course. They are kind of related but definitely not the same. All that being said, I don't know much about what they study. My only point was that, to get into one of those subs, they had to be in the top 2-3% of a fairly competitive bunch of students. Just getting into dental school is competitive and then you skim the top couple percent off of that group and you likely are dealing with some pretty bright, motivated, and competitive candidates.
That has always been my argument of why an anesthesiologist is inherently better than a CRNA. Because we have had several layers of weedout processes. Getting into college, getting into pre med program, not "washing out" of pre med program with the highest level science courses, taking the MCAT, getting into med school, passing all of your courses, getting into a residency program, getting board certified., etc. Every single step was high stakes and had the potential to end the journey for you.
Conversely, CRNAs have getting into college (often junior college night classes), taking lower tier science classes that non science majors take, getting accepted to nursing school (pretty much anyone who has a B average is successful), and maintaining grades in clinicals. Working a year in ICU following a doctor's prescribed orders, and paying the money to get into CRNA school, then doing the equivalent of a 30 minute grand rounds literature search as your dissertation on a topic such as PONV. Then take your "boards" with a 99+% pass rate (100 questions and they tell you right then and there if you pass). Think about it. The only high stakes exam they ever take is their board exam, which has a 99+% pass rate.
So, with physicians, you are getting the best of the best students at a baseline. With nursing, you are getting students who will pass through the process almost always once they decide they wish to do it. The biggest hurdle is the getting into nursing school and that is almost always assured unless you are a terrible student. There are so many CRNA programs that, if you are willing to take on the debt, they will let you in as soon as they have an open spot as long as you have done your 1 year ICU time. The debt has become quite large and that has caused many to shy away from tackling the process at the current time, so schools are being less selective in who they choose.
Meanwhile, dental students have had the same scrutiny and weedout processes that mded students have with a few differences. So, I would argue that the dental students are likely at a far superior level of baseline smarts.
My theory is that there are a few CRNAs that are better at anesthesia than the bottom tier physicians, but the vast majority of physicians are superior as a baseline.
View attachment 366370

 forums.studentdoctor.net
forums.studentdoctor.net
never going to happen. its foolish to think we will win this battle with evidence. when the other side isnt playing fair.Its going to be more and more important that we have solid, unbiased evidence of our outcome superiority. We need data that any idiot with any knowledge of research methodology can't shoot a million holes in. ASA - hope you're listening.
Our best evidence to date came out last year and the ASA has done ****-all to advertise it, hype it or institute guidelines to that effect.Its going to be more and more important that we have solid, unbiased evidence of our outcome superiority. We need data that any idiot with any knowledge of research methodology can't shoot a million holes in. ASA - hope you're listening.
 jamanetwork.com
jamanetwork.com
Cadavers work for credentialing.Simulated procedures can count toward procedure logs for EM. At least they could 7 years ago when I interviewed. Even in a big, busy department they’re probably doing a single digit number of crics per year as a group. There’s no way some program with 12-15 residents per year is getting everyone 3 crics on real patients in 3 years. Likewise with pericardioscentesis. Where I did residency they had done 1 in the prior calendar year as a department when I rotated through as an intern.
Sorry, I cannot agree with that statement. Anyone with a research degree and any understanding of anesthesia is going to pick this study to pieces because of the methodology.Our best evidence to date came out last year and the ASA has done ****-all to advertise it, hype it or institute guidelines to that effect.
If the ASA had any balls, they'd come out with guidelines damning ratios greater than 3:1. But too many fat cats would have to change their models for that to happen.
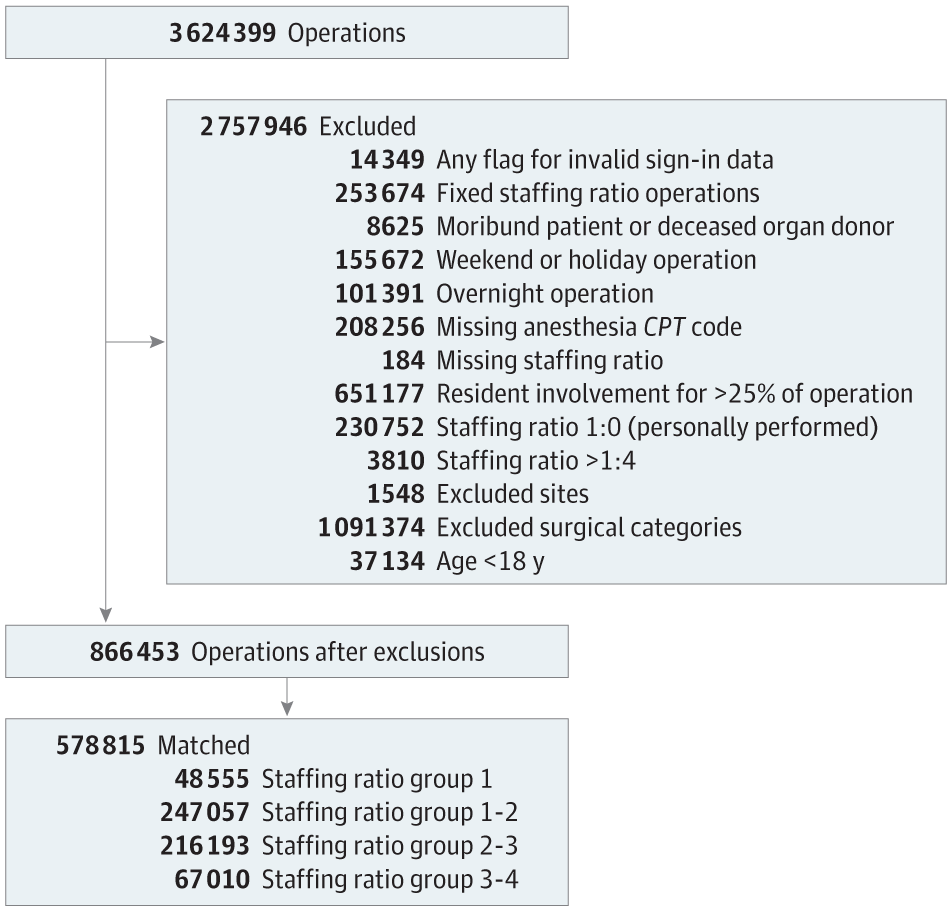
Anesthesiologist Staffing Ratio and Surgical Patient Morbidity and Mortality
This cohort study uses data from the Multicenter Perioperative Outcomes Group database to examine the association between intraoperative anesthesiologist staffing ratio and surgical patient morbidity and mortality across 23 hospitals in 18 states.
I’m supervising OMFS residents and they scare the shiiii out of meOn the IQ and got-their-****-together bell curves, OMFS residents are faaaaaar to the right of the NP-wannabes. Yeah, you can make a good CA1 out of an OMFS resident (for appropriately selected cases) but I don't get where you think that level of trainability translates to the pool of nurses who want to be NPs.
OMFS is populated by one of the most talented and driven cohorts of people in healthcare. Yeah. They do great. Of course they do. So what?
Are you not similarly "scared" by CA1s in months 0-6?I’m supervising OMFS residents and they scare the shiiii out of me
did you read the papers published in nursing journal about how crna provide equivalent care? what do you think about those studies? just curiousSorry, I cannot agree with that statement. Anyone with a research degree and any understanding of anesthesia is going to pick this study to pieces because of the methodology.
The issues are:
1) The 1:1 supervision group had the highest absolute mortality, highest % of ASA 1 patients and lowest % of ASA 3 patients
2) They excluded cases with typically lower supervision ratios and higher complications (after hours, cardiac, liver transplant)
3) They excluded cases with typically higher supervision ratios and fewer complications (cataracts, OB)
4) They didn't completely eliminate residents
5) They didn't include physician only and CRNA only care
6) They used propensity scoring (obviously cant risk stratify in a retrospective sample) but comorbidity % was higher in many key areas for higher ratio cases.
FFS guys this looks like it was designed specifically to create the result they wanted. This is what I meant by "any idiot with a research degree shooting a million holes in". We've got to do better
did you read the papers published in nursing journal about how crna provide equivalent care? what do you think about those studies? just curious
but in the end, i dont really care about methodology or whatever at this point. because the other side doesnt play fair. many people will just read the headlines. when crnas publish a paper saying crnas provide better care than MD, and if NYT picks up on it, they arent going to dissect it. the headline itself will be a win for them. at this point its all about wins.
if you are going to a no weapons war, and the other side brings guns. what will you do? say thats not fair, they broke the rules, and continue fighting with your fists and die, or are you going to get some guns? i think its time ASA get some guns
Yes lolAre you not similarly "scared" by CA1s in months 0-6?
Are you not similarly "scared" by CA1s in months 0-6?
The decision-makers are going to look at all the data on both sides and say "this is all flawed", then make the decision they want to make anyway. The ratios study is no different - it looks like it was designed with the end in mind, whether or not that was the intent. Would be nice to have something more comprehensive and controlled that nobody can argue with. Hospital c-suites don't give a crap about us or them, they just want to spend the least while maintaining qualityWe are too proud (dumb) to play dirty. As one of my family members who was in politics used to say, “when the other side play dirty, you need to play dirtier to win.” I used to think that’s a very bleak way to look at situations.
As the healthcare systems, insurance companies, hospitals and midlevels gunning for us, we are standing at the same spot yelling “we need a randomized controlled study to prove this is true…..” just boggles my mind.
The decision-makers are going to look at all the data on both sides and say "this is all flawed", then make the decision they want to make anyway. The ratios study is no different - it looks like it was designed with the end in mind, whether or not that was the intent. Would be nice to have something more comprehensive and controlled that nobody can argue with. Hospital c-suites don't give a crap about us or them, they just want to spend the least while maintaining quality
nah they want want to spend the least amount of money providing a quality of care they can get away with.The decision-makers are going to look at all the data on both sides and say "this is all flawed", then make the decision they want to make anyway. The ratios study is no different - it looks like it was designed with the end in mind, whether or not that was the intent. Would be nice to have something more comprehensive and controlled that nobody can argue with. Hospital c-suites don't give a crap about us or them, they just want to spend the least while maintaining quality
The ratios study is no different - it looks like it was designed with the end in mind, whether or not that was the intent. Would be nice to have something more comprehensive and controlled that nobody can argue with.
As much as the AANA would like to discredit this study, it was well-designed and the results match what every anesthesiologist would expect. This was a huge study of 600,000 cases.Anyone with a research degree and any understanding of anesthesia is going to pick this study to pieces because of the methodology.
The issues are:
1) The 1:1 supervision group had the highest absolute mortality, highest % of ASA 1 patients and lowest % of ASA 3 patients
2) They excluded cases with typically lower supervision ratios and higher complications (after hours, cardiac, liver transplant)
3) They excluded cases with typically higher supervision ratios and fewer complications (cataracts, OB)
4) They didn't completely eliminate residents
5) They didn't include physician only and CRNA only care
6) They used propensity scoring (obviously cant risk stratify in a retrospective sample) but comorbidity % was higher in many key areas for higher ratio cases.
FFS guys this looks like it was designed specifically to create the result they wanted. This is what I meant by "any idiot with a research degree shooting a million holes in". We've got to do better
Fixed it for you.Hospital c-suites don't give a crap about us or them, they just want to spend the leastwhile maintaining quality
There is no “we”. Just a bunch of individuals currently enjoying a great job market and hoping the gravy train keeps chugging along. This specialty has always selected for the type B “go along, get along” types. To think we would ever fight is naive in the extreme….We are too proud (dumb) to play dirty. As one of my family members who was in politics used to say, “when the other side play dirty, you need to play dirtier to win.” I used to think that’s a very bleak way to look at situations.
As the healthcare systems, insurance companies, hospitals and midlevels gunning for us, we are standing at the same spot yelling “we need a randomized controlled study to prove this is true…..” just boggles my mind.
There is no “we”. Just a bunch of individuals currently enjoying a great job market and hoping the gravy train keeps chugging along. This specialty has always selected for the type B “go along, get along” types. To think we would ever fight is naive in the extreme….
How do mid-levels feel comfortable in whatever field they work in? It takes years of residency and working to know how to safely practice and recognize conditions. How does an RN out of NP school without a lick of clinical experience know what the hell to do... Heck I don't feel comfortable to be doing anything other than what I practice, yet they can bounce around to any and every specialty and can do it all!That can be said about any hospital based field. (EM, Hospitalist, consulting services for GI, ID, cardiology….). Aren’t they sort of coming to derm? That’s also why this conversation is happening in this particular thread. History likes to repeat itself. This is just another warning for “us”. Here’s the road map how they gutted EM, and they’re coming for us (those who will still be practicing in 20 years, left to hold the bag).
Sure “it’s too late”, “they already sold this field out….”; There are still thriving MD only practices, they’re are practices who will do 1:3 max supervision. And most if not all of us oppose CRNA independence, under the current payment scheme. So there some common grounds that we can all work on.
Responding to your points:As much as the AANA would like to discredit this study, it was well-designed and the results match what every anesthesiologist would expect. This was a huge study of 600,000 cases.
1- If there's any hidden confounding here; it's in the opposite direction of what you're alleging. Why would a MD supervise a nurse 1:1? Because the nurse sucks or because the patient is sick.
There was no statistical difference in the ASA composition of any of the groups. (Table 2). The threshold for standardized difference was set at 0.2-- all were below 0.05. It seems odd that you cherry-picked the raw numbers of ASA 3's for your claim. Did you not also see that Group 1 was tied for the highest number of ASA 4's and had the second-highest emergency cases?
2&3- They explained this in the Methods-- they purposefully excluded operations that have fixed staffing ratios.
4- They excluded cases in which residents were present more than 25% of the time-- look at the MPOG member sites (https://mpog.org/).They're all academic centers. The vast majority of these cases have some resident involvement. Is your argument that residents are surreptitiously killing patients and then handing them over to CRNAs?
5- That wasn't the aim of the study. Again, look at the MPOG member sites. How many of these do you think are providing MD only or CRNA-only cases? They're 99% ACT model.
If its so obvious that this was a bad study, then why don't you write an editorial to the ASA or JAMA?
How do mid-levels feel comfortable in whatever field they work in? It takes years of residency and working to know how to safely practice and recognize conditions. How does an RN out of NP school without a lick of clinical experience know what the hell to do... Heck I don't feel comfortable to be doing anything other than what I practice, yet they can bounce around to any and every specialty and can do it all!
How do mid-levels feel comfortable in whatever field they work in? It takes years of residency and working to know how to safely practice and recognize conditions. How does an RN out of NP school without a lick of clinical experience know what the hell to do... Heck I don't feel comfortable to be doing anything other than what I practice, yet they can bounce around to any and every specialty and can do it all!
Or they order every test known to man, costing much more than the money saved to avoid paying for that pesky physician.They might feel comfortable but that doesnt mean they have the same competency. They always have someone to help them with complicated issues or they refer them out.
You should certainly be scared to be hospitalized for any reason. So long as the person has a license (brand new NP or PA) the hospital will be happy to hire.Or they order every test known to man, costing much more than the money saved to avoid paying for that pesky physician.
In residency had a brought a young patient s/p VATS intubated, with plan for extubation in ICU. On way to CVICU pt looking like he wanted to fast track his recovery, so I told the nurse give reversal and just extubate since he met criteria anyway. Instead the ICU NP said they don't reverse patients, and instead put him on a prop drip and cardene infusion for his elevated BP and heart rate and thrashing instead of just pulling the tube. Mismanagement to the max. I have so many stories of much more mismanagement by our top of the license "colleagues"
I'm truly scared to get sick and be in any hospital, and be subject to the "care" they subject patients to