- Joined
- Apr 3, 2019
- Messages
- 5,178
- Reaction score
- 11,768
- Points
- 5,601
- Attending Physician

I dunno; did oncotype have prospective data when it entered routine practice?Will first need to be validated in a prospective randomized clinical trial. Once it is, I do expect this to change management and radonc volume significantly.
It will be nice to have something definitive to hang my hat on and say "this is why you need breast RT".
I dunno; did oncotype have prospective data when it entered routine practice?
Imagine this will be ordered by med oncs and surgeons who will then not send the low risk patients.
Not to say any of the above is right, but probably how it will go down.
Recommend Multi-D clinic/discussion prior to surgery if logistically possible.That would be so frustrating to be cut out of the loop without even a word to say
However there is precedent - look at pancreas, lymphoma
We would have to rely on the lazy surgeons/medoncs that dump to radonc "for discussion"
That would be so frustrating to be cut out of the loop without even a word to say
However there is precedent - look at pancreas, lymphoma
We would have to rely on the lazy surgeons/medoncs that dump to radonc "for discussion"
In the long run surgeons aren't going to send us all their breast patients for "discussion" once they realize those with a low score don't need to be inconvenienced/confused by having said "discussion." See above examples regarding pancreas and lymphoma.
Dont they already have something similar for OncotypeDX DCIS? Feels like uptake for that has been pretty low
Also the long term updates on all these studies always show the curves widening the most after 10 years
View attachment 364193
Party is just getting started. More personalized biomarkers/Ct dna will follow.I dunno; did oncotype have prospective data when it entered routine practice?
Imagine this will be ordered by med oncs and surgeons who will then not send the low risk patients.
Not to say any of the above is right, but probably how it will go down.
Pretty much any post op indication could be fair game eventuallyParty is just getting started. More personalized biomarkers/Ct dna will follow.
I think this is where we're headed. Gonna take a while to get there. But post op indications in 10 years gonna look a LOT different.Party is just getting started. More personalized biomarkers/Ct dna will follow.
We'll be treating half the patients as today with twice the doctors! UnbelievableI think this is where we're headed. Gonna take a while to get there. But post op indications in 10 years gonna look a LOT different.
Great use of personalized medicine to spare patients unnecessary treatment if validated.
Terrible foresight / greed by the senior and leaders of our field to have no mechanism or rationale discussion to modify number of trainees as indications and fractions shrink. Breast is a large driver of how we benefit society. Without that, society needs less of us. But we are training more of us. Golden parachutes for the old guard!
That's one take. Another take is, if there's no indication for RT, there's no need for a #radonc to be in the loop.That would be so frustrating to be cut out of the loop without even a word to say
As it should be, imho (if there's agreed to be no need for RT).In the long run surgeons aren't going to send us all their breast patients for "discussion" once they realize those with a low score don't need to be inconvenienced/confused by having said "discussion."
That is probably going to be true, but sometimes a standard sets foot as a standard (at least in the eyes of surgeons/med oncs) before NCCN declares it a standard. I don't recall if NCCN explicitly says don't do radiation in low-risk older women with breast cancer, but it's standard in the eyes of many:I would think that this surgeon ordering the test phenomenon won't take off too much until the test enters NCCN guidelines.
Dont they already have something similar for OncotypeDX DCIS?

That would be logical.Breast is a large driver of how we benefit society. Without that, society needs less of us.
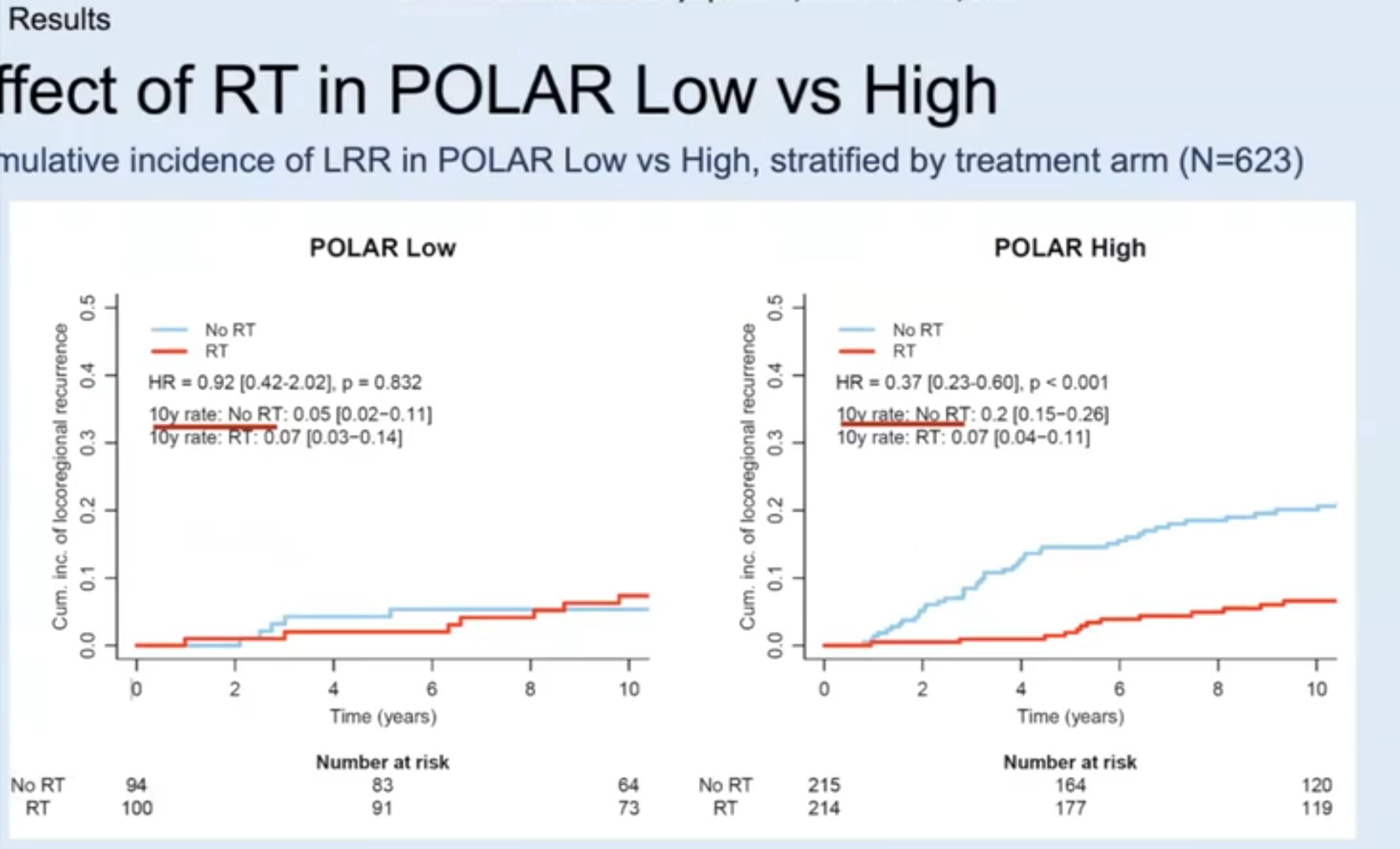
It looks like curve for POLAR-low and getting RT will separate for higher local failure after 10y vs no RT.Also the long term updates on all these studies always show the curves widening the most after 10 years
“How can we minimize morbidity while preserving outcomes for locally advanced rectal cancer?… There are a few ways that we can approach this. The first is omission of radiation.”Pretty much any post op indication could be fair game eventually


 www.medpagetoday.com
www.medpagetoday.com
“How can we minimize morbidity while preserving outcomes for locally advanced rectal cancer?… There are a few ways that we can approach this. The first is omission of radiation.”
Forego Radiotherapy for Women With Low-Risk Luminal A Breast Cancer?
Study shows 5-year local recurrence rate of 2.3% with lumpectomy and endocrine therapy alone
“Corey speers MD, PhD, of the University of Michigan in Ann Arbor. "It really is a personalized approach to identifying these patients. Identifying these patients based on their intrinsic molecular subtype of the tumor, based on the biology, and not just clinical and pathological features, suggests we can really identify these patients who are at very low risk of their cancer coming back."
a lot of curves look like a lot of things when presented as small unpublished abstracts, good thing we have trials and statisticsIt looks like curve for POLAR-low and getting RT will separate for higher local failure after 10y vs no RT.
The Lord giveth, and the Lord separateth away.
That's one take. Another take is, if there's no indication for RT, there's no need for a #radonc to be in the loop.
As it should be, imho (if there's agreed to be no need for RT).
That is probably going to be true, but sometimes a standard sets foot as a standard (at least in the eyes of surgeons/med oncs) before NCCN declares it a standard. I don't recall if NCCN explicitly says don't do radiation in low-risk older women with breast cancer, but it's standard in the eyes of many:
What I see as a possibility: one day... it will just change. POLAR will become standard. And rad onc's won't really be consulted about the change or be part of the change one way or the other.
That would be logical.
It looks like curve for POLAR-low and getting RT will separate for higher local failure after 10y vs no RT.
The Lord giveth, and the Lord separateth away.
“How can we minimize morbidity while preserving outcomes for locally advanced rectal cancer?… There are a few ways that we can approach this. The first is omission of radiation.”

That's one take. Another take is, if there's no indication for RT, there's no need for a #radonc to be in the loop.
As it should be, imho (if there's agreed to be no need for RT).
That is probably going to be true, but sometimes a standard sets foot as a standard (at least in the eyes of surgeons/med oncs) before NCCN declares it a standard. I don't recall if NCCN explicitly says don't do radiation in low-risk older women with breast cancer, but it's standard in the eyes of many:
What I see as a possibility: one day... it will just change. POLAR will become standard. And rad onc's won't really be consulted about the change or be part of the change one way or the other.
That would be logical.
It looks like curve for POLAR-low and getting RT will separate for higher local failure after 10y vs no RT.
The Lord giveth, and the Lord separateth away.
“How can we minimize morbidity while preserving outcomes for locally advanced rectal cancer?… There are a few ways that we can approach this. The first is omission of radiation.”
If you thinking running retrospective analysis on prospective clinical trials is the stuff that scientific revolutions are made out of, ...
Pan-cancer prediction of radiotherapy benefit using genomic-adjusted radiation dose (GARD): a cohort-based pooled analysis
The biological effect of radiotherapy, as quantified by GARD, is significantly associated with time to first recurrence and overall survival for patients with cancer treated with radiation. It is predictive of radiotherapy benefit, and physical dose of radiation is not. We propose integration of...www.thelancet.com
they should do a study looking at patient reported QOL of endocrine therapy vs. RT.How about the benefit of not having to do 5 years of HRT?
I'm can't discern any meaningful value to GARD. The type of thing that is appealing on the surface, but not meaningful in practice. GARD is gonna tell me to give 50 or 60 Gy? Please.If you think running retrospective analysis on prospective clinical trials is the stuff that scientific revolutions are made out of, then you must have lost your mind when you saw this
Pan-cancer prediction of radiotherapy benefit using genomic-adjusted radiation dose (GARD): a cohort-based pooled analysis
The biological effect of radiotherapy, as quantified by GARD, is significantly associated with time to first recurrence and overall survival for patients with cancer treated with radiation. It is predictive of radiotherapy benefit, and physical dose of radiation is not. We propose integration of...www.thelancet.com
No no no. Not saying that. I am saying Oncology is a Culture (intentional capitalization). And scientific revolution is about culture and cultural changes and the humans that drive change and not so much about science and data and proof (not as much as one would think). And increasingly rad onc is not participating and driving the Culture of Oncology but more like "logs floating in the stream of life." I am speaking to Kuhn's "paradigms." For radiation oncologists e.g. it is yet to be seen if the "oligometastatic paradigm" is a Kuhnian paradigm; it's not looking favorable imho.If you think running retrospective analysis on prospective clinical trials is the stuff that scientific revolutions are made out of, then you must have lost your mind when you saw this
Pan-cancer prediction of radiotherapy benefit using genomic-adjusted radiation dose (GARD): a cohort-based pooled analysis
The biological effect of radiotherapy, as quantified by GARD, is significantly associated with time to first recurrence and overall survival for patients with cancer treated with radiation. It is predictive of radiotherapy benefit, and physical dose of radiation is not. We propose integration of...www.thelancet.com
Use of "they" here is what I'm getting at above; the "they" is Oncology. And "they" will not let this study be a new paradigm even if it shows LC's are going to be similar. Just being real. And we know they would be similar, we don't even need that study... there's reasonable enough data already to suggest such a study's outcome.they should do a study looking at patient reported QOL of endocrine therapy vs. RT.
The Culture of Oncology! It seems weird to us. But we are rad oncs maybe not in tune with the Culture.I love weird editorials and this is up there for sure!
It's just inevitable. There are radoncs who are true molecular researchers and are very much involved in driving oncology culture. Everyone else, not so much. To the degree that we have "an agenda" with our research to support our lone intervention, we will never be players. To the degree that we are open minded with our research, we will continue to undermine our lone intervention.And increasingly rad onc is not participating and driving the Culture of Oncology but more like "logs floating in the stream of life."
Respectfully: why do you prescribe 60 Gy? Is there any biological basis to that decision? Or is it because it is an arbitrary dose that we've always done for Stage # (fill in the blank) cancer?I'm can't discern any meaningful value to GARD. The type of thing that is appealing on the surface, but not meaningful in practice. GARD is gonna tell me to give 50 or 60 Gy? Please.
That you Jake 🙂Respectfully: why do you prescribe 60 Gy? Is there any biological basis to that decision? Or is it because it is an arbitrary dose that we've always done for Stage # (fill in the blank) cancer?
Cause it's worked (meaning demonstrated some disease control benefit with acceptable toxicity) in large groups of patients and neither dose escalation nor de-escalation trials have indicated better clinical outcomes.Respectfully: why do you prescribe 60 Gy? Is there any biological basis to that decision? Or is it because it is an arbitrary dose that we've always done for Stage # (fill in the blank) cancer?
No no no. Not saying that. I am saying Oncology is a Culture (intentional capitalization). And scientific revolution is about culture and cultural changes and the humans that drive change and not so much about science and data and proof (not as much as one would think). And increasingly rad onc is not participating and driving the Culture of Oncology but more like "logs floating in the stream of life." I am speaking to Kuhn's "paradigms." For radiation oncologists e.g. it is yet to be seen if the "oligometastatic paradigm" is a Kuhnian paradigm; it's not looking favorable imho.
Don't feel like it's telling tales out of school to observe that The Culture of Oncology is heavy into rad onc minimization right now.
Use of "they" here is what I'm getting at above; the "they" is Oncology. And "they" will not let this study be a new paradigm even if it shows LC's are going to be similar. Just being real. And we know they would be similar, we don't even need that study... there's reasonable enough data already to suggest such a study's outcome.
The Culture of Oncology! It seems weird to us. But we are rad oncs maybe not in tune with the Culture.
I like and welcome the optimism but oversupply isn’t good. It’s like having an oversupply of termites or syphilllis.I am not sure I buy this idea that intentional omission of radiation is some new thing signaling an age where rad onc is actively being minimized. People have always tried to come up with ways to eliminate or reduce RT, and its not even new for breast (the oncotype dx DCIS data has been around for over a decade at this point) and people have been doing RT breast omission studies since breast RT became a standard of care.
To me, trying to keep breast and prostate as our bread and butter and clinging on to how things have always been done is a surefire way to become "logs floating in the stream of life." Rad onc is changing, oversupply is real, and there is not likely going to be a "soft landing" for people not willing/able to adapt with the changing landscape of oncology. Conversely, I actually think an overall larger pool of rad oncs is actually going to help the field in the long, long term (not salary wise though unfortunately). The smaller the specialty we are, the easier it would be for the rest of oncology to leave us behind. But the fact its, we have a bigger footprint manpower wise than we ever have had and its up to us on how to best leverage that going forward
Don’t you mean catfish?I like and welcome the optimism but oversupply isn’t good. It’s like having an oversupply of termites or syphilllis.
We are increasing supply by opening unnecessary, objectively weak programs becoming the easiest specialty in the match for US grads to match intoI am not sure I buy this idea that intentional omission of radiation is some new thing signaling an age where rad onc is actively being minimized. People have always tried to come up with ways to eliminate or reduce RT, and its not even new for breast (the oncotype dx DCIS data has been around for over a decade at this point) and people have been doing RT breast omission studies since breast RT became a standard of care.
To me, trying to keep breast and prostate as our bread and butter and clinging on to how things have always been done is a surefire way to become "logs floating in the stream of life." Rad onc is changing, oversupply is real, and there is not likely going to be a "soft landing" for people not willing/able to adapt with the changing landscape of oncology. Conversely, I actually think an overall larger pool of rad oncs is actually going to help the field in the long, long term (not salary wise though unfortunately). The smaller the specialty we are, the easier it would be for the rest of oncology to leave us behind. But the fact its, we have a bigger footprint manpower wise than we ever have had and its up to us on how to best leverage that going forward
I am not sure I buy this idea that intentional omission of radiation is some new thing signaling an age where rad onc is actively being minimized. People have always tried to come up with ways to eliminate or reduce RT, and its not even new for breast (the oncotype dx DCIS data has been around for over a decade at this point) and people have been doing RT breast omission studies since breast RT became a standard of care.
To me, trying to keep breast and prostate as our bread and butter and clinging on to how things have always been done is a surefire way to become "logs floating in the stream of life." Rad onc is changing, oversupply is real, and there is not likely going to be a "soft landing" for people not willing/able to adapt with the changing landscape of oncology. Conversely, I actually think an overall larger pool of rad oncs is actually going to help the field in the long, long term (not salary wise though unfortunately). The smaller the specialty we are, the easier it would be for the rest of oncology to leave us behind. But the fact its, we have a bigger footprint manpower wise than we ever have had and its up to us on how to best leverage that going forward
This is absolutely hilarious for a multitude of reasons. We all know surgeons and the chemo doctors would never in a million years allow a study that will enable omission of their modality although a similar study would easily validate omission of chemo and/or surgery in probably at least 30-40% of malignancies.
I’m cracking up here picturing a bunch of bow tied ROS with rabbinical knowledge of every breast ca study published seething silently and impotently in their usual back seats of the breast MDT while surgeons and the chemo doctors continue to push their treatment with no credible evidence except the same shoddy studies handed to them by drug reps.
If you asked 10000 women what they found more helpful and more tolerable between RT and any form of systemic therapy not one would say they would raise their head in support of the chemo doctors.
We have known for more than 50 years that definitive Rt for early breast gives us the exact same control rates as WLE +RT but we choose to intentionally omit the most important single therapy from management. LMAO. Not a single trial looking at definitive RT in the population and omission of surgery, even though the Japanese are getting equivalent for SABR in the cohort. Laughable.
At the end of the day patients lose and locoregional control rates lose. The chemo guys get more patients and inflict more misery upon women. We continue to be pushed around by people in our profession who wouldn’t even be allowed into medical school in a rational world. Clown world indeed, folks.
They're all the worst now.Breast is the worst!
I offer it quite a bit. If a woman is concerned about being compliant with 5 years of an AI, i tell them a short course of RT becomes even more important to considerI see no reason why an early stage er+ grade elderly couldn't have hypofractionated RT only? Addition of surgery unlikely to provide benefit. Surely one can devise a validation program for this?
I am not sure I buy this idea that intentional omission of radiation is some new thing signaling an age where rad onc is actively being minimized. People have always tried to come up with ways to eliminate or reduce RT, and its not even new for breast (the oncotype dx DCIS data has been around for over a decade at this point) and people have been doing RT breast omission studies since breast RT became a standard of care.
To me, trying to keep breast and prostate as our bread and butter and clinging on to how things have always been done is a surefire way to become "logs floating in the stream of life." Rad onc is changing, oversupply is real, and there is not likely going to be a "soft landing" for people not willing/able to adapt with the changing landscape of oncology. Conversely, I actually think an overall larger pool of rad oncs is actually going to help the field in the long, long term (not salary wise though unfortunately). The smaller the specialty we are, the easier it would be for the rest of oncology to leave us behind. But the fact its, we have a bigger footprint manpower wise than we ever have had and its up to us on how to best leverage that going forward
What in the hell are you babbling about?


I mean, couldn't we offer hypofractionatedRT only, as in no surgery as valid option? I have never had a woman choose ET or RT in the setting.I offer it quite a bit. If a woman is concerned about being compliant with 5 years of an AI, i tell them a short course of RT becomes even more important to consider