I mentioned that during his first surgery significant IE burden was found, including on the subvalvular apparatus....which at the time required extensive chordal resection.
Keep in mind that the totality of the mitral apparatus (annulus, leaflets, chords, paps), not just LV myocardium, is required for physiologic LV systolic function, and the LV really does not like it when its constituents are disrupted.
"The importance of preserving the mitral valve
apparatus in maintaining normal left ventricular mechanics and contractile function has been further emphasized in several experimental and clinical studies.
These studies demonstrated that disrupting the chordae tendineae caused a reduction in contraction in left ventricular segments adjacent to the papillary muscles, a less spherical geometry during isovolumic systole, a more spherical geometry at end systole, and a reduction in contractile state."
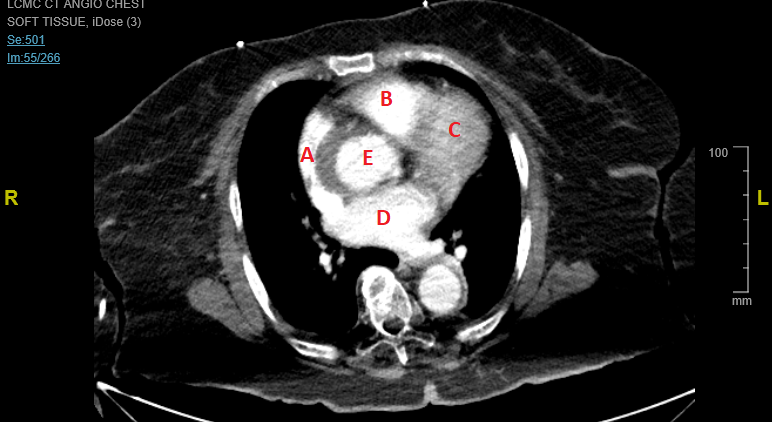
Think of the locations of the
posteromedial and
anterolateral papillary muscles...now you know why his function is decreased with clean coronaries but in a specific RWMA pattern.




![umg]](/proxy.php?image=https%3A%2F%2Fi.imgur.com%2FF5mV1Lr.gif%5B%2Fumg%5D&hash=d31c8d8e2ef72cc9af630a218c0e0c51)